

Abstract
Context:
Rapid stretching of the skin over the weak connective tissue leads to development of striae distensae. Recently, researchers have shown special interest towards use of fractional photothermolysis in treatment of striae and several studies have shown its usefulness. Our aim was to assess the efficacy of Fractional CO2 laser in treatment of striae alba.
Materials and Methods:
A randomized clinical trial was carried out in female patients with striae alba. Ninety two striae were randomly selected and divided into two groups. Five sessions of laser resurfacing, were performed in Group 1, every 2–4 weeks. Group 2 was treated with 10% glycolic acid+0.05% tretinoin cream nightly during the study. Photographs were taken from the striae before and two weeks after the end of treatment. Mean surface area of striae compared between two groups. Patients’ views regarding the degree of improvement were assessed via visual analogue scale (VAS).
Results:
Forty six striae in Group 1 underwent laser resurfacing and 46 matched striae in Group 2, were treated with topical cream. Mean difference of striae surface area, was significantly decreased after treatment in Group 1 (-37.1±15.6 cm2) in comparison with Group 2(-7.9±9 cm2) (P value >0.001). Mean VAS was significantly higher in Group 1 (3.05±0.74) compared to Group 2 (0.63±0.66) (P value >0.001).
Conclusions:
Fractional photothermolysis via Fractional CO2 laser seems to be an effective method for treatment of striae alba.
Keywords: Fractional photothermolysis, fractional CO2 laser, striae alba, striae distensae
INTRODUCTION
Rapid stretching of the skin over the weak connective tissue in the dermis leads to development of linear scars, which are called striae distensae (SD) or stretch marks.[1]
Striae distensae are found in all races and are usually located on the buttocks, thighs, knees, calves and lumbosacral areas.[2]
Causes of striae distensae are not fully understood and several theories like tissue damage by striatoxin, mechanical stretching and rupture of connective tissue framework, pregnancy, normal growth, especially in adolescents, rapid weight change and high serum levels of steroids, are proposed.[3,4]
SD is 2.5 times as frequent in women and is commonly seen in 90% of pregnant women.[3] SD is common in adolescence and pregnancy. SD in pregnancy at first develops in abdomen and then involves the breasts too.[4]
Clinically, SD in early-stage are pink or red in color (striae rubra) but over time and with atrophic changes they become white (striae alba).[5]
The histology of SD is similar to a scar and development of SD is similar to wound healing or scar formation.[6]
Several treatments for SD have been suggested but no consistent treatment modality has been established yet.[3,7]
Laser resurfacing is one of the favorite treatment modalities for striae. It seems that effect of laser in treatment of striae is via collagen increase in extracellular matrix.[3]
Fractional photothermolysis stimulates epidermal turn over and dermal collagen remodeling, which leads to significant improvement in several types of scars[8–10] and has been approved by FDA for treatment of different kinds of scars.[3] According to histological similarities of striae alba and scar, recently researchers have shown special interest towards use of fractional photothermolysis in treatment of striae, especially striae alba[3,11,12] and several studies have shown that it is useful in treatment of striae.[3,11–18]
We designed this study to assess the effect of fractional photothermolysis using Fractional CO2 laser in treatment of striae alba, for the first time in our patients with skin types III-IV in Iran.
MATERIALS AND METHODS
This study was a randomized clinical trial, carried out in the patients who referred to Novin Laser Center in Isfahan, Iran in 2010. Subjects were selected via simple random sampling method. Patients with striae alba on abdomen, buttocks and flanks who had never received any previous treatment for SD and had skin type III-IV, were included in this study.
Exclusion criteria were: Pregnancy, breast feeding, striae alba on chest or arms, previous medical or laser therapy for SD, and history of topical or systemic steroid use, Cushing or Ehlers-Danlos syndrome, isotretinoin use, filler injection, dermabrasion or laser skin resurfacing in past 6–12 months in the area of SD.[18]
This study was approved by Ethic Committee of Isfahan University of Medical Sciences (Research project number: 388432) and written consent was obtained from all of the participants, before starting the study.
Six participants who met the inclusion criteria were selected, all of them were female considering the fact that SD is more prevalent in them and most patients who seek cosmetic treatments for SD are women. In each patient pairs of striae alba with similar shape and size and approximately symmetrical site, were selected.
Totally, 92 striae in 6 participants were selected and divided into two matched groups, with 46 striae in each. Left sided and right sided striae were randomly selected to be enrolled in either group. In some patients, the striae of the left side were treated by laser resurfacing and in the others the striae on the right side.
Group 1 was treated with Fractional CO2 laser resurfacing and Group 2 with 10% glycolic acid+0.05% tretinoin cream.
Topical treatment of striae distensae with 0.1% Tretinoin cream is a proven modality.[19] Result of another study showed that topical glycolic acid can modify the appearance of striae distensae but is better used in combination with other topical treatments.[19,20] In one study, 15% glycolic acid has been used with 0.05% tretinoin and proven effective.[19] Since, tretinoin cream is a proven treatment for striae distensae and glycolic acid, especially in combination with other topical agents is effective to improve the appearance of striae, we decided to use 10% glycolic acid in combination with 0.05% tretinoin cream in order to prevent excessive skin irritation and burning that could adversely affect the patients’ compliance. In each patient, half of the selected striae, were treated with Fractional CO2 laser and the other half, were treated with 10% glycolic acid+0.05% tretinoin cream.
Before and after treatment, shape of every striae was drawn on the oil paper and surface area of each striae was measured and recorded by placing the transparent oil paper with the shape of each striae on the 5 mm graph paper and counting the number of squares contributing to a given shape. Surface area of a given striae was measured by multiplying the number of squares by 25 mm2 (surface area of each square).
Topical lidocaine cream was applied on the skin under occlusion, 60 min before laser therapy. Then laser resurfacing was done by an experienced dermatologist using Fractional CO2 laser (Qray FRX, DOSIS M and M CO., LTD). The instrument characteristics are as follows:
Laser type: Ultra pulse, 10600 nm
CO2 tube: All metal sealed off waveguide RF tube
Output energy: 140 mJ
Pulse duration: 20–9540 μs
Scanning size: 3×3 mm to 20×20 mm
Density: 0.5–2.0 mm
Scan mode: Standard, Refresh, Breeze, Chill, Double and Scatter.
Our chosen setting was: Laser Fluence: 16 ± 2 J/cm2, Dot cycle: 5 ± 2, Pixel pitch: 0.8 ± 0.1. Laser therapy was done for 5 sessions at 2-4-week intervals and at every session we used 2 laser passes.[21] During the operation, skin residuals were removed from the site of laser therapy with wet sterile gauze.
If the patients complained of severe erythema and edema or if any evidence of post-inflammatory hyperpigmentation (PIP) was seen after laser therapy, we would change our laser setting by lowering the fluence, decreasing Dot cycle or increasing Pixel pitch.
Participants were advised to clean the site of laser therapy with sterile normal saline solution, apply mupirocin and zinc oxide ointment and use sterile Vaseline gauze following resurfacing procedure.
In each visit, we assessed any complication (persistent erythema, post-inflammatory hypo- and hyperpigmentation and scar formation) and if there were any complication, we would change our laser setting accordingly.
All of the participants were recommended to apply 10% glycolic acid+0.05% tretinoin cream nightly, as long as being treated by laser (10–20 weeks), on the striae of opposite site of the body which had not been treated by laser resurfacing. Starting with nightly application of short contact (1 h) in the first week, the patients were recommended to gradually increase the duration of contact by 15 min in each application during the second week, by the 3rd week the patients were asked to apply the cream for longer duration, as long as they could tolerate, at most until the next morning.
Participants were followed up every other week until two months after treatment.
Digital photographs were taken from all of the striae (via Canon IXUS 210), before initiation and two weeks after finishing of both treatment modalities.
Photographs were assessed by two non-treating dermatologists who were not aware of the used treatment modalities in this study. The percent of improvement was determined according to the following assessment scale:
At the end of the study, patients’ views regarding the degree of improvement in both treatment modalities were assessed via visual analogue scale (VAS).
VAS is a ten-point self-assessment scale, which measures a special characteristic or conception in a spectrum between zero and ten.[22,23]
According to this scale, zero means no improvement and 10 means complete improvement in our study.
Data were analyzed via SPSSv19/win, using independent and paired t-test and ANCOVA.
RESULTS
Totally, 92 striae were selected and divided into two groups with 46 striae in each, in 6 patients based on the inclusion criteria. Forty six striae in Group 1 were treated with Fractional CO2 laser and 46 matched striae in Group 2 (in symmetrical position on the other side of the body) were treated with 10% glycolic acid+0.05% tretinoin cream. On the other hand in each patient, half the selected striae were enrolled in Group 1 and the other half on the opposite side were enrolled in Group 2.
The variables of our study are surface area of striae Before treatment (SAB), surface area of striae after treatment (SAA), visual analogue scale (VAS), dermatologist assessed improvement scale (DIS), and surface area difference (d.SA = SAA-SAB).
Table 1 shows that no significant difference in mean surface area of striae before treatment (SAB) was seen between two groups using independent t-test (P value=0.82), implying the presumed condition that the striae of the 2 groups should have almost same shape and size.
Table 1.
Mean surface area before (SAB) and after (SAA) treatment modalities, Mean surface area difference (d.SA), Mean VAS and DIS in both groups
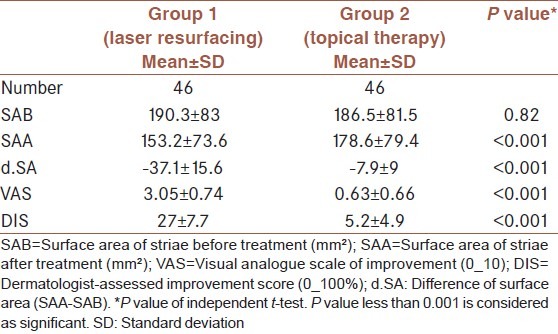
Results of this study showed that the mean surface area of striae after treatment (SAA) in both groups was decreased after treatment [Table 1].
The mean SAA did not show significant difference in Group 1 in comparison with Group 2 using independent t-test, but considering the fact that surface area of striae before treatment in Group 1 was a bit larger than Group 2 (190 mm2 vs. 186 mm2) and in in order to omit the confounding effect of this difference, we used Analysis of Covariance (ANCOVA) test, which showed that the mean SAA in Group 1, which underwent laser therapy was significantly decreased in comparison with Group 2 (P value >0.001). It means laser therapy was more effective in decreasing the surface area of striae than topical therapy [Table 1].
The mean surface area difference (d.SA) showed significant difference in Group 1 in comparison with Group 2 (P value >0.001), it means that laser therapy decreased the surface area of striae significantly more than topical therapy [Table 1].
The mean VAS and the mean DIS, were significantly higher in Group 1 (P value>0.001) [Table 1]. It means, both patients and dermatologists found laser therapy more effective in improving the appearance of striae alba.
Table 2 shows that surface area of striae significantly decreased in Group 1, which underwent laser resurfacing using paired t-test (P value, 0.001). It means that laser was effective in decreasing the surface area of striae.
Table 2.
Mean surface area before (SAB) and after (SAA) treatment within each group
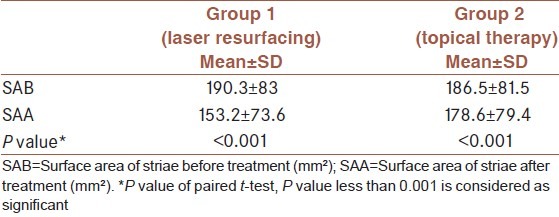
The surface area of striae significantly decreased in Group 2, which received topical treatment (P value >0.001, paired t-test). It means that topical therapy is also effective in decreasing surface area of striae.
Figure 1 shows the significant improvement of striae alba after laser therapy in comparison with topical therapy with 10% glycolic acid+0.05% tretinoin cream [Figure 2].
Figure 1.
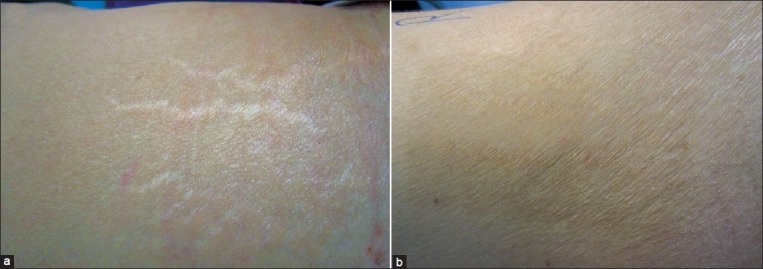
Striae distensae on the right flank of a representative patient. Show significant improvement at 12 weeks post-treatment: (a) at baseline; (b) after 5 sessions of fractional photothermolysis
Figure 2.
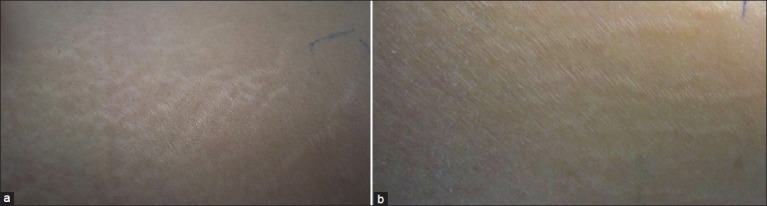
Striae distensae on the left flank of the same patient. Show relative improvement at 12 weeks post-treatment: (a) at baseline; (b) after 3 month treatment with 10% glycolic acid+0.05% tretinoin cream
Only one participant had developed post-inflammatory hyperpigmentation in two-month fallow-up, who was treated with hydroquinone cream.
DISCUSSION
Among different modalities for treatment of striae distensae, fractional photothermolysis is a novel method.[3,12,13,18]
Fractional resurfacing laser has been approved by FDA for treatment of acne scars in 2006. This system ablates a fraction of the skin leaving regions of normal skin to repopulate the ablated columns.[3,24]
Different studies have reported the efficacy of fractional photothermolysis in treatment of various types of scars.[3,11,25]
Considering the similar histological characteristics in striae alba and scars and successful treatment of scars using fractional photothermolysis, recently researchers have shown special interest towards the use of fractional photothermolysis for improvement and treatment of SD, especially striae alba.[3,11]
Until now results of few studies regarding treatment of striae with fractional photothermolysis have been published.[3]
Our study showed that decrease of surface area of striae was significantly more after laser resurfacing with Fractional CO2 laser, compared with topical therapy using 10% glycolic acid+0.05% tretinoin (P value >0.001). These results also showed that although topical therapy within group two had significant effect in improvement of striae alba but Group 1, which underwent fractional photothermolysis had more significant improvement.
Macedo et al. study showed successful results in treatment of striae alba via 1550 nm Fraxel SL Laser.[3] We used Fractional CO2 laser(10600 nm) but both studies showed efficacy of fractional photothermolysis in treatment of striae alba.
A Korean study reported that fractional photothermolysis both histologically and visually had significant effect in treatment of striae gravidarum without any side effect.[12]
Our study showed fractional photothermolysis has a visually significant effect in treatment of striae alba, which matches the results of this Korean study. In both studies the participants were female, and no serious side effects were observed but in our study, different types of striae distensae including striae gravidarum were treated.
Lee et al. study showed that fractional CO2 laser (10600 nm) has a positive effect on late stage striae distensae, which is similar to our results. In both studies, the type of fractional photothermolysis was similar (CO2 laser) and all the participants were female. In Lee et al. study the skin type was Fitzpatrick IV and only one session of laser was done but in our study skin types were III and IV and 5 sessions of laser therapy were performed.[18]
Kim et al. study reported that 1550-nm erbium-doped FP laser, made remarkable macroscopic and histological improvement in striae alba.[13] Results of Kim et al. study is similar to ours. In both studies 6 female participants were enrolled and only mild hyperpigmentation in some of the participants developed but laser systems in these two studies were different, and the striae were not histologically assessed in our study.
Stotland et al. showed positive effect of 1550-nm erbium-doped fiber laser in treatment of both striae alba and striae rubra.[14]
Bak et al. study reported that fractional photothermolysis significantly improves striae alba which resembles our results.[15]
A recent study by de Angelis et al. showed safety and efficacy of fractional non-ablative 1540 nm erbium: Glass laser in treatment of striae alba and rubra[16] which is close to our results although laser systems and sample sizes were different but duration of both studies was the same.
The limitation of the present study is the lack of histological assessment.
The current study concluded that fractional photothermolysis via Fractional CO2 laser is an effective and safe method for treatment of striae alba in patients with skin types III-IV. More studies on effect of Fractional CO2 laser in treatment of SD are suggested.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.McDaniel DH. Laser therapy of stretch marks. Dermatol Clin. 2002;20:67–76, viii. doi: 10.1016/s0733-8635(03)00046-9. [DOI] [PubMed] [Google Scholar]
- 2.Cho S, Park ES, Lee DH, Li K, Chung JH. Clinical features and risk factors for striae distensae in Korean adolescents. J Eur Acad Dermatol Venereol. 2006;20:1108–13. doi: 10.1111/j.1468-3083.2006.01747.x. [DOI] [PubMed] [Google Scholar]
- 3.Elsaie ML, Baumann LS, Elsaaiee LT. Striae distensae (stretch marks) and different modalities of therapy: An update. Dermatol Surg. 2009;35:563–73. doi: 10.1111/j.1524-4725.2009.01094.x. [DOI] [PubMed] [Google Scholar]
- 4.Burrows NP, Lovell CR. Disorders of connective tissue. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook’s Textbook of Dermatology. 8th ed. Oxford: Wiley-Blackwell; 2010. p. 455. [Google Scholar]
- 5.Hermanns JF, Piérard GE. High-resolution epiluminescence colorimetry of striae distensae. J Eur Acad Dermatol Venereol. 2006;20:282–7. doi: 10.1111/j.1468-3083.2006.01426.x. [DOI] [PubMed] [Google Scholar]
- 6.Atwal GS, Manku LK, Griffiths CE, Polson DW. Striae gravidarum in primiparae. Br J Dermatol. 2006;155:965–9. doi: 10.1111/j.1365-2133.2006.07427.x. [DOI] [PubMed] [Google Scholar]
- 7.Taavoni S, Soltanipour F, Haghani H, Ansarian H, Kheirkhah M. Effects of olive oil on striae gravidarum in the second trimester of pregnancy. Complement Ther Clin Pract. 2011;17:167–9. doi: 10.1016/j.ctcp.2010.10.003. [DOI] [PubMed] [Google Scholar]
- 8.Alster TS, Tanzi EL, Lazarus M. The use of fractional laser photothermolysis for the treatment of atrophic scars. Dermatol Surg. 2007;33:295–9. doi: 10.1111/j.1524-4725.2007.33059.x. [DOI] [PubMed] [Google Scholar]
- 9.Hasegawa T, Matsukura T, Mizuno Y, Suga Y, Ogawa H, Ikeda S. Clinical trial of a laser device called fractional photothermolysis system for acne scars. J Dermatol. 2006;33:623–7. doi: 10.1111/j.1346-8138.2006.00143.x. [DOI] [PubMed] [Google Scholar]
- 10.Behroozan DS, Goldberg LH, Dai T, Geronemus RG, Friedman PM. Fractional photothermolysis for the treatment of surgical scars: A case report. J Cosmet Laser Ther. 2006;8:35–8. doi: 10.1080/14764170600607251. [DOI] [PubMed] [Google Scholar]
- 11.Shin JU, Roh MR, Rah DK, Ae NK, Suh H, Chung KY. The effect of succinylated atelocollagen and ablative fractional resurfacing laser on striae distensae. J Dermatolog Treat. 2011;22:113–21. doi: 10.3109/09546630903476902. [DOI] [PubMed] [Google Scholar]
- 12.Yang YJ, Lee GY. Treatment of Striae Distensae with Nonablative Fractional Laser versus Ablative CO(2) Fractional Laser: A Randomized Controlled Trial. Ann Dermatol. 2011;23:481–9. doi: 10.5021/ad.2011.23.4.481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kim BJ, Lee DH, Kim MN, Song KY, Cho WI, Lee CK, et al. Fractional photothermolysis for the treatment of striae distensae in Asian skin. Am J Clin Dermatol. 2008;9:33–7. doi: 10.2165/00128071-200809010-00003. [DOI] [PubMed] [Google Scholar]
- 14.Stotland M, Chapas AM, Brightman L, Sukal S, Hale E, Karen J, et al. The safety and efficacy of fractional photothermolysis for the correction of striae distensae. J Drugs Dermatol. 2008;7:857–61. [PubMed] [Google Scholar]
- 15.Bak H, Kim BJ, Lee WJ, Bang JS, Lee SY, Choi JH, et al. Treatment of striae distensae with fractional photothermolysis. Dermatol Surg. 2009;35:1215–20. doi: 10.1111/j.1524-4725.2009.01221.x. [DOI] [PubMed] [Google Scholar]
- 16.De Angelis F, Kolesnikova L, Renato F, Liguori G. Fractional nonablative 1540-nm laser treatment of striae distensae in Fitzpatrick skin types II to IV: Clinical and histological results. Aesthet Surg J. 2011;31:411–9. doi: 10.1177/1090820X11402493. [DOI] [PubMed] [Google Scholar]
- 17.Alexiades-Armenaka M, Sarnoff D, Gotkin R, Sadick N. Multi-center clinical study and review of fractional ablative CO 2 laser resurfacing for the treatment of rhytides, photoaging, scars and striae. J Drugs Dermatol. 2011;10:352–62. [PubMed] [Google Scholar]
- 18.Lee SE, Kim JH, Lee SJ, Lee JE, Kang JM, Kim YK, et al. Treatment of striae distensae using an ablative 10,600-nm carbon dioxide fractional laser: A retrospective review of 27 participants. Dermatol Surg. 2010;36:1683–90. doi: 10.1111/j.1524-4725.2010.01719.x. [DOI] [PubMed] [Google Scholar]
- 19.Ash K, Lord J, Zukowski M, McDaniel DH. Comparison of topical therapy for striae alba (20% glycolic acid/0.05% tretinoin versus 20% glycolic acid/10% L-ascorbic acid) Dermatol Surg. 1998;24:849–56. doi: 10.1111/j.1524-4725.1998.tb04262.x. [DOI] [PubMed] [Google Scholar]
- 20.Mazzarello V, Farace F, Ena P, Fenu G, Mulas P, Piu L, et al. A superficial texture analysis of 70% glycolic acid topical therapy and striae distensae. Plast Reconstr Surg. 2012;129:589e–90e. doi: 10.1097/PRS.0b013e3182419c40. [DOI] [PubMed] [Google Scholar]
- 21.Walia S, Alster TS. Prolonged clinical and histologic effects from CO 2 laser resurfacing of atrophic acne scars. Dermatol Surg. 1999;25:926–30. doi: 10.1046/j.1524-4725.1999.99115.x. [DOI] [PubMed] [Google Scholar]
- 22.Schick U, Elhabony R. Prospective comparative study of lumbar sequestrectomy and microdiscectomy. Minim Invasive Neurosurg. 2009;52:180–5. doi: 10.1055/s-0029-1237379. [DOI] [PubMed] [Google Scholar]
- 23.Gould D, Kelly D, Goldstone L, Gammon J. Examining the validity of pressure ulcer risk assessment scales: Developing and using illustrated patient simulations to collect the data. J Clin Nurs. 2001;10:697–706. doi: 10.1046/j.1365-2702.2001.00525.x. [DOI] [PubMed] [Google Scholar]
- 24.Alexiades-Armenakas MR, Dover JS, Kenneth AA. Laser therapy. In: Bolognia JL, Jorizzo JL, Rapini RP, editors. Dermatology. 2nd ed. St. Louis (MO): Mosby Elsevier; 2008. p. 2113. [Google Scholar]
- 25.Glaich AS, Goldberg LH, Friedman RH, Friedman PM. Fractional photothermolysis for the treatment of postinflammatory erythema resulting from acne vulgaris. Dermatol Surg. 2007;33:842–6. doi: 10.1111/j.1524-4725.2007.33180.x. [DOI] [PubMed] [Google Scholar]