
Figure 1.
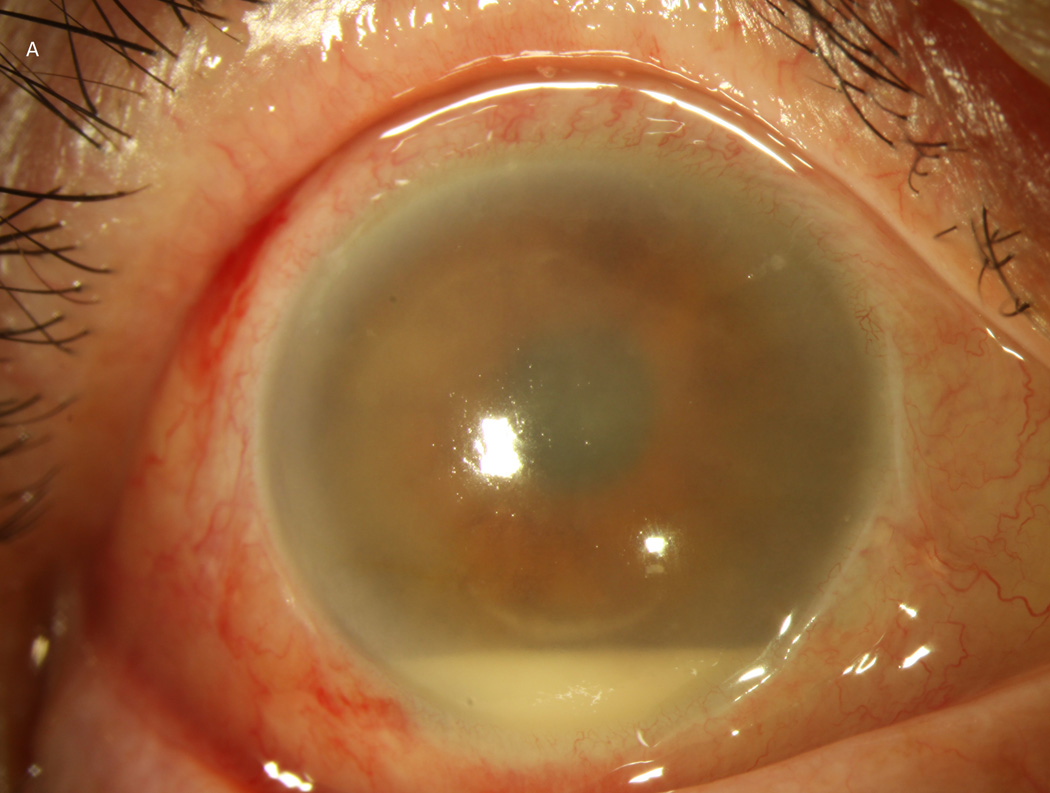

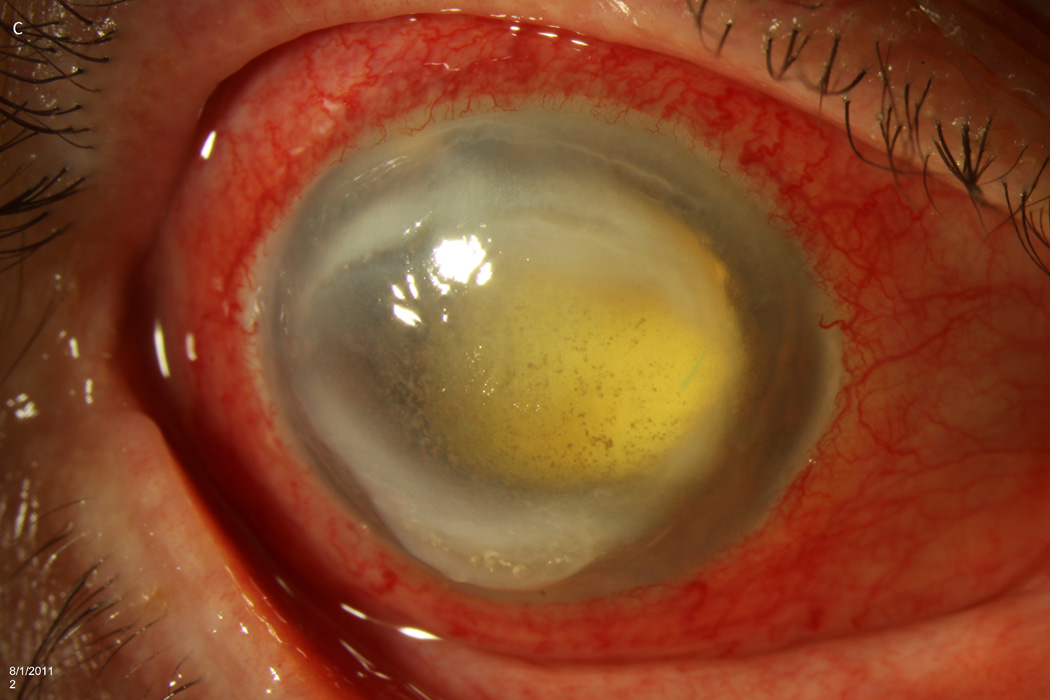
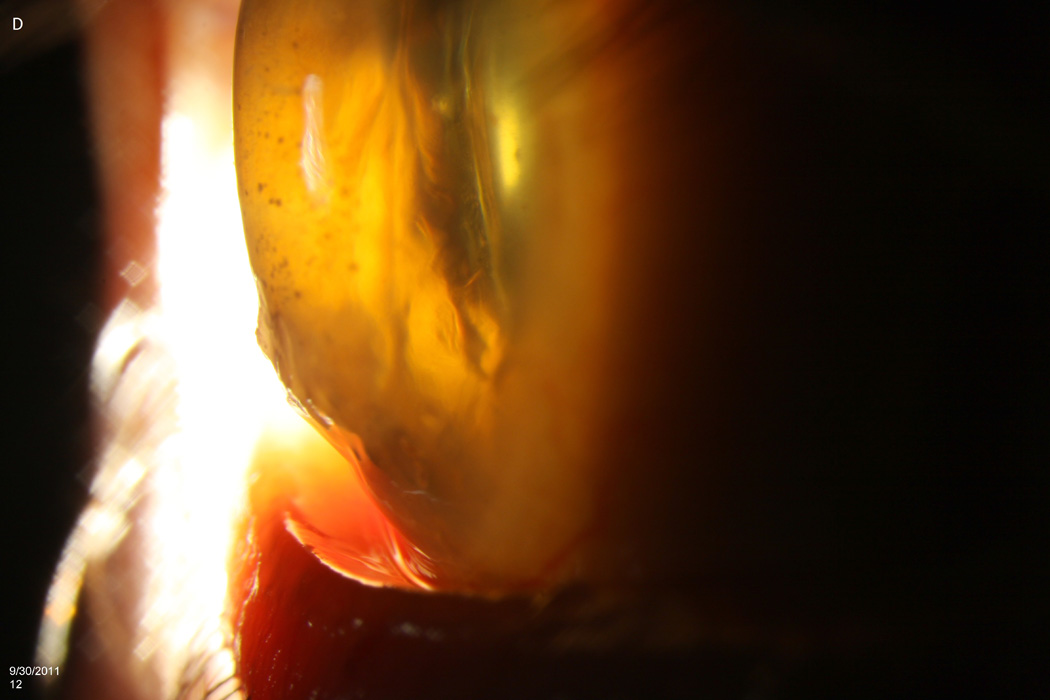
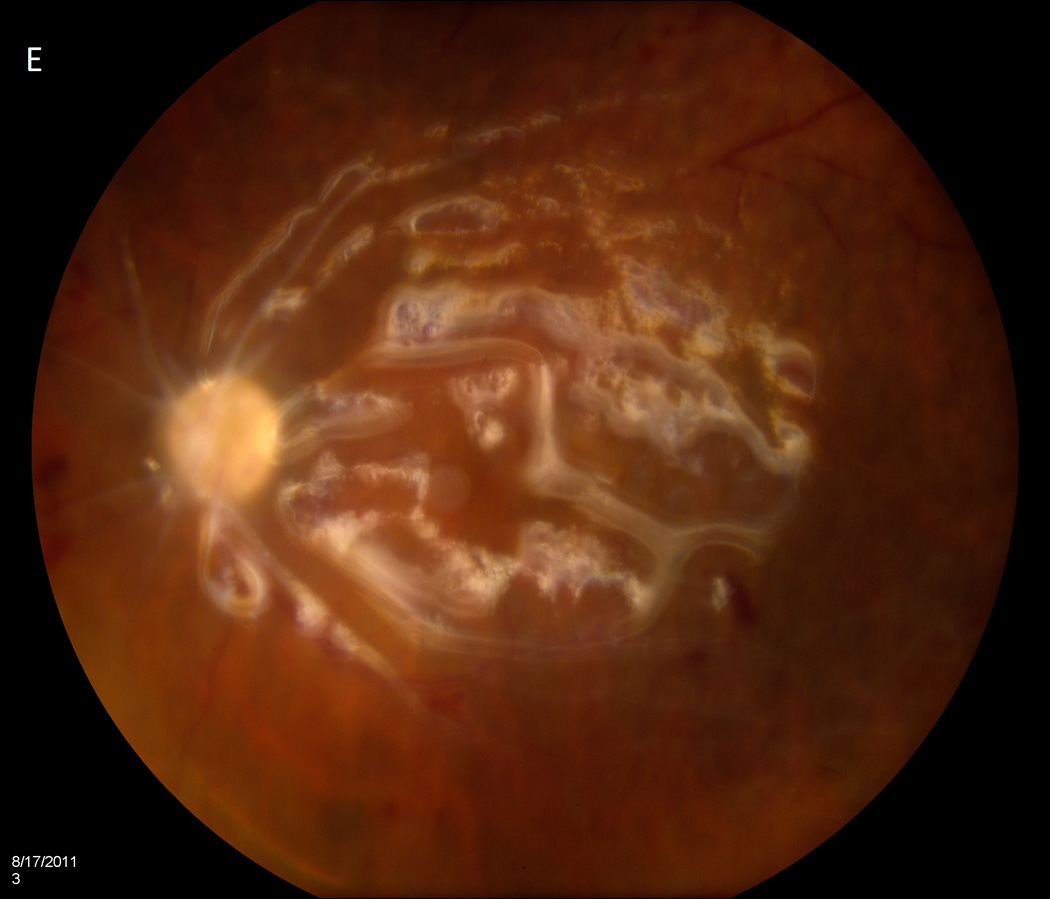
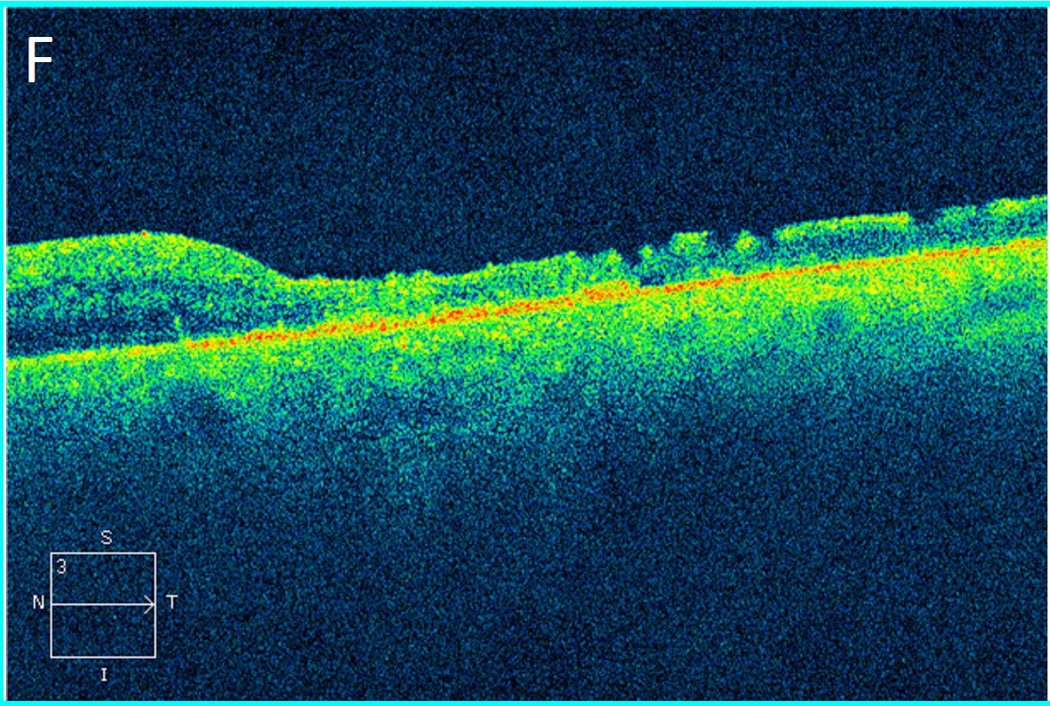
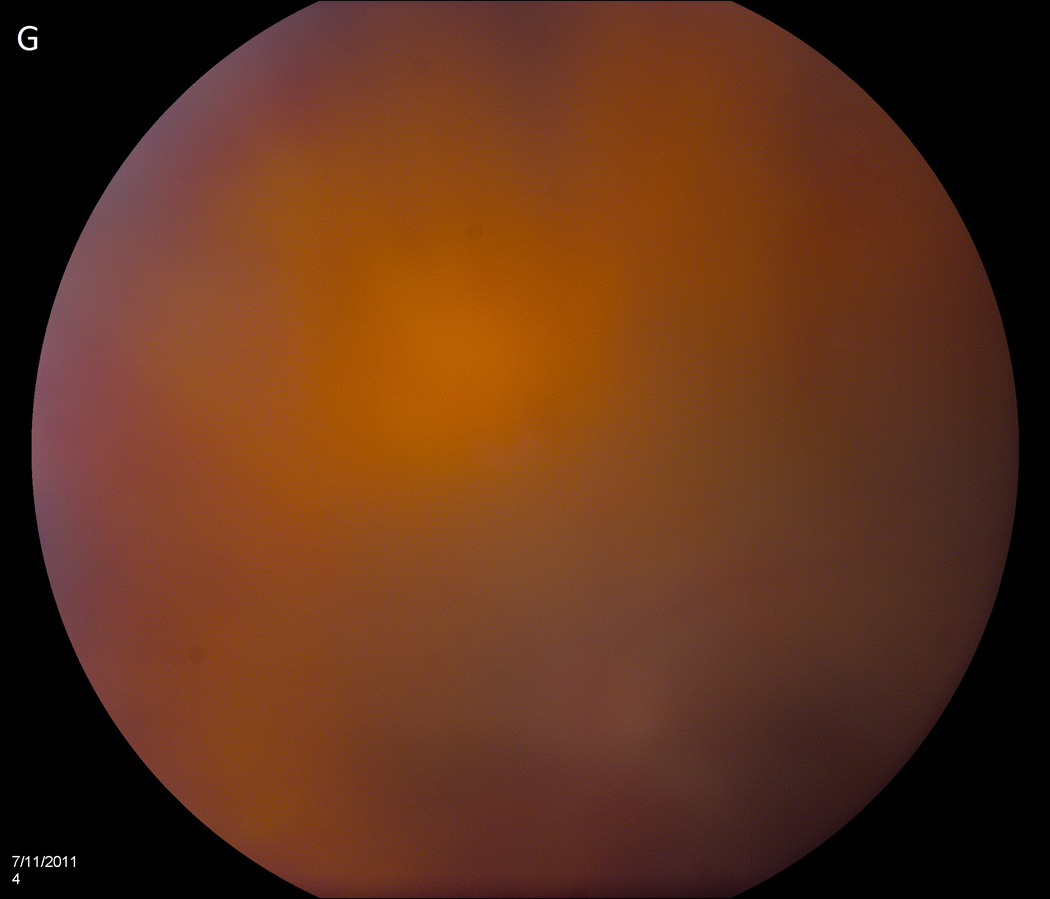
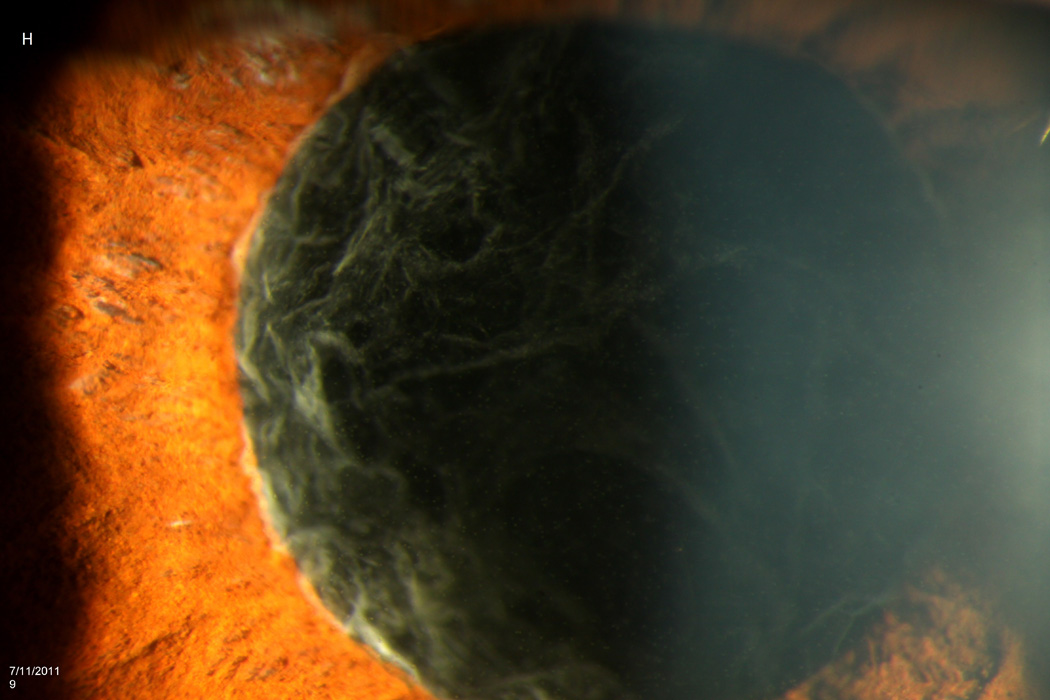
Case 2 demonstrates the marked anterior chamber reaction and a layered hypopyon (A) that most patients presented with. Echography obtained at that time confirmed the presence of a dense vitritis with prominent membranes (B). As the inflammation consolidated, several patients developed a dense ring infiltrate (C) which, in Case 8, left a prominent inferior ectasia in the cornea (D). When the view cleared sufficiently to allow for pars plana vitrectomy, the optic nerves were often pale, the vessels sclerosed, and the retina atrophic, as in Case 3 (E, F). Case 7 was the only patient to be regain her pre-injection visual acuity. She presented 3 days after her injection with milder signs and symptoms than the other patients. Her Snellen visual acuity had deteriorated from 20/40 to 20/200, with a hazy vitritis (G) and prominent pupillary fibrin (H).