

Icodextrin is a starch-derived glucose polymer that has been on the European market since the 1990s. It is used by more than 10 000 peritoneal dialysis (PD) patients worldwide because it provides sustained positive net ultrafiltration during the long dwell and better metabolic control than that provided by glucose-based solutions, especially in diabetic PD patients (1,2). Furthermore, positive associations with patient and technique survival have been demonstrated for icodextrin (3).
Baxter Healthcare Corporation has the only marketing authorization for icodextrin and manufactures it in plants both inside Europe (Ireland, Turkey) and outside Europe (United States, Canada, Singapore). In Europe, icodextrin is labeled with a purple-colored cap.
At our department, PD patients normally use 7.5% icodextrin solution manufactured at the Baxter plant in Castlebar, Ireland. Because of elevated endotoxin levels in some PD solution bags manufactured at that plant (4), our patients treated with continuous ambulatory PD were switched temporarily in the early part of 2011 to icodextrin solution produced in Turkey. For automated PD, icodextrin was imported from the US manufacturing plant.
Although all 7.5% icodextrin solutions contain the same colloid osmotic agent, there might have been differences between the bags obtained from the various plants at that time. We illustrate this possibility with the following case report and spiking experiment.
Case Description
A 65-year-old man with a history of diabetes mellitus, hypertension, and an acute coronary syndrome started continuous ambulatory PD in October 2010. He used a dialysis schedule of 3 exchanges with a 2.27% glucose-based solution (Physioneal: Baxter Healthcare Corporation) during the day and icodextrin (Extraneal 7.5%: Baxter Healthcare Corporation) during the night. In January 2011, his 7.5% icodextrin bags, normally from the Castlebar plant, were replaced with bags from Turkey after a special importation exemption was established to meet the clinical needs of patients across Europe.
During use of the Turkish 7.5% icodextrin solution, our patient noticed a purple discoloration of the bag in the very early drainage phase (Figure 1). Within 30 seconds, the discoloration disappeared, probably because of dilution. He had never noticed this discoloration while using icodextrin produced in Ireland. We suspected that this discoloration was related to the presence of iodine in the PD disconnect cap, and so we decided to test our hypothesis by injecting povidone iodine into two unused 7.5% icodextrin bags from different plants. After injection of 1 mL 10% povidone iodine into a 7.5% icodextrin bag manufactured in Turkey, a purple discoloration occurred [Figure 2(A)] that persisted for at least 1 hour [Figure 2(B)]. After injection of 1 mL 10% povidone iodine into a 7.5% icodextrin bag manufactured in Ireland, a brown discoloration was observed [Figure 2(C)], which quickly disappeared [Figure 2(D)].
Figure 1.

— Purple discoloration of an icodextrin bag in the very early drainage phase.
Figure 2.
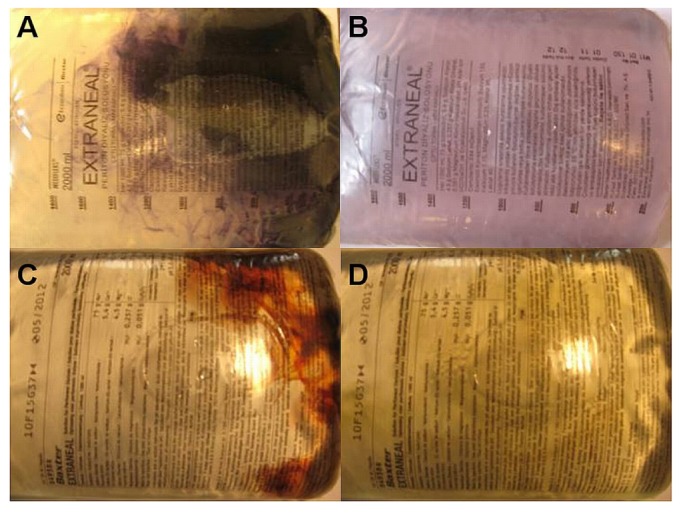
— Color results after injection of 10% povidone iodine 1 mL into unused 7.5% icodextrin bags from different manufacturing plants. (A,B) The immediate purple discoloration of fluid from the plant in Turkey persists for at least 1 hour. (C,D) The immediate brownish-red discoloration of fluid from the plant in Ireland quickly disappears.
In June 2011, our patient switched to automated PD, for which he used 7.5% icodextrin solution manufactured in the United States for the long daytime dwell. No purple discoloration has been seen since that time.
Discussion
Icodextrin is derived from cornstarch. The two major components of starch are amylose and amylopectin. Amylose consists mainly of long linear chains of α-1,4 linked glucose molecules (typically 200 - 20 000 units), which form helices. Amylopectin is a highly branched molecule of shorter α-1,4 glucose residues and more frequent α-1,6 branches. Amylopectin molecules may contain up to two million glucose units.
The ratio between amylose and amylopectin depends on the starch source. Cornstarch consists of about 30% amylose and 70% amylopectin, but waxy corn contains only amylopectin and no amylose (5).
Amylose is responsible for the classic blue-black color seen after starch comes into contact with iodine, probably because I3- and I5- ions fit inside the amylose helix. That complex has energy-level spacings that correspond to the absorption spectrum in visible light. Amylopectin does not form a complex with iodine and does not induce the typical blue-black color reaction (5).
Maltodextrin, formed by enzymatic hydrolyzation of pure starch, is used as the raw material for the production of icodextrin. Maltodextrins consist of d-glucopyranose polymers of various chain length, linked by α-(1-4) and α-(1-6) glucosidic bonds. In the production of icodextrin, maltodextrin is fractionated by dissolving it in purified water and passing it sequentially through two ultrafiltration membrane stacks. The result is a polydispersed mixture of polymers consisting of 2 - 300 glucose molecules, of which more than 85% have a molecular weight between 1640 Da and 45 000 Da (6).
Until 2011, the raw maltodextrin used to make icodextrin solutions for patients in Europe was supplied by two different vendors. Since then, all maltodextrin has come from a single vendor.
Blue-black discoloration of icodextrin solutions has been reported earlier (7-9). In those reports, the discoloration was attributed to the reaction between povidone iodine present in the disconnect cap and constituents of the icodextrin solution and was postulated to be similar to the usual reaction between iodine and starch. Our case report and spiking experiment add to those observations and show that the composition of icodextrin 7.5% bags varied depending on the plant in which they has been manufactured.
Iodine causes a black-blue color reaction when added to solutions containing polymers of 20 or more glucose molecules (10). Otherwise, a brownish-red discoloration occurs, similar to that seen when adding povidone iodine to saline- or glucose-containing PD fluid. Consequently, our observation indicates that, compared with icodextrin solutions manufactured in other plants, icodextrin produced in Turkey contained more polymers consisting of more than 20 molecules of glucose. The difference is attributable to the different composition of the maltodextrin stock used at that time.
The clinical significance of our finding is not known. However, patients and caregivers should be aware of the brown or purple discoloration that may appear when draining icodextrin from the abdomen after use of a iodine-containing disconnect cap.
Disclosures
No grant support was received for the present work. ACA has received clinical grants from Baxter Healthcare Corporation. PR is Medical Director (Renal) of Baxter Healthcare SA for Europe, Middle East, and Africa. WHB has no financial conflicts of interest to declare.
References
- 1. Qi H, Xu C, Yan H, Ma J. Comparison of icodextrin and glucose solutions for long dwell exchange in peritoneal dialysis: a meta-analysis of randomized controlled trials. Perit Dial Int 2011; 31:179–88 [DOI] [PubMed] [Google Scholar]
- 2. Paniagua R, Ventura MD, Avila-Díaz M, Cisneros A, Vicenté-Martínez M, Furlong MD, et al. Icodextrin improves metabolic and fluid management in high and high-average transport diabetic patients. Perit Dial Int 2009; 29:422–32 [PubMed] [Google Scholar]
- 3. Han SH, Ahn SV, Yun JY, Tranæus A, Han DS. Effects of icodextrin on patient survival and technique success in patients undergoing peritoneal dialysis. Nephrol Dial Transplant 2012; 27:2044–50 [DOI] [PubMed] [Google Scholar]
- 4. European Medicines Agency (EMA) Questions and Answers on Endotoxins in Dialysis Solutions Produced at Baxter Manufacturing Plant. London, UK: EMA; 2011. [Available online at: http://www.ema.europa.eu/docs/en_GB/document_library/Medicine_QA/2011/01/WC500101074.pdf; accessed 30 July 2012] [Google Scholar]
- 5. Pérez S, Bertoft E. The molecular structure of starch components and their contribution to the architecture of starch granules: a comprehensive review. Starch/Stärke 2010; 62:389–420 [Google Scholar]
- 6. Alsop RM. History, chemical and pharmaceutical development of icodextrin. Perit Dial Int 1994; 14(Suppl 2):S5–12 [Google Scholar]
- 7. Robertson S, Huxtable H, Blakemore C, Williams G, Donovan KL. The icodextrin black line sign. Perit Dial Int 2001; 21:621–3 [PubMed] [Google Scholar]
- 8. Camilleri B, Glancey G, Pledger D, Williams P. The icodextrin black line sign to confirm a pleural leak in a patient on peritoneal dialysis. Perit Dial Int 2004; 24:197 [PubMed] [Google Scholar]
- 9. Sekercioglu N, Jassal SV. Early morning blues—a complication of icodextrin. Perit Dial Int 2004; 24:197–9 [PubMed] [Google Scholar]
- 10. Bailey JM, Whelan WJ. Physical properties of starch. I. Relationship between iodine stain and chain length. J Biol Chem 1961; 236:969–73 [PubMed] [Google Scholar]