
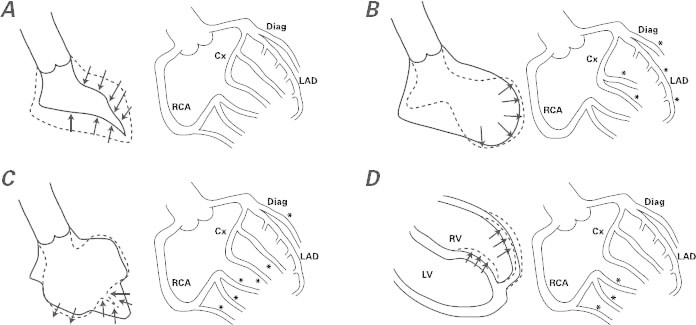
Fig. 4 Side-by-side diagrams illustrate ventricular patterns of regional dysfunction at the end of an endothelial function test performed when the left ventricular (LV) dysfunction has mostly resolved (usually 3–7 d after onset). Findings by LV angiography appear in A–C (at the left in each figure) and by cardiovascular magnetic resonance in D (again at left), and the corresponding coronary angiographic findings after acetylcholine testing appear in A–D (at the right in each figure), according to our group's theory and the early results of acetylcholine testing. A) Negative acetylcholine test, observed in patients with normal endothelial function. B) Apical ballooning seen in typical takotsubo syndrome, accompanied by severe spasm (asterisks) at most of the left-sided, epicardial branches on acetylcholine testing. (Small vessels in these territories are also affected.) C) The effect of acetylcholine infusion on the branches of the left coronary artery in a case of mid-ventricular takotsubo. The middle segments of the LV are dyskinetic at the same time that most branches, except for the left anterior descending coronary artery (LAD), are severely obstructed. D) Right ventricular (RV) apical dyskinesia and isolated right coronary artery (RCA) spasm at acetylcholine testing in a case of RV takotsubo. Usually, RV takotsubo occurs jointly with apical LV takotsubo, as in panel B.
*Site of severe spasm
Cx = circumflex coronary artery; Diag = diagonal coronary artery