
Figure 2.
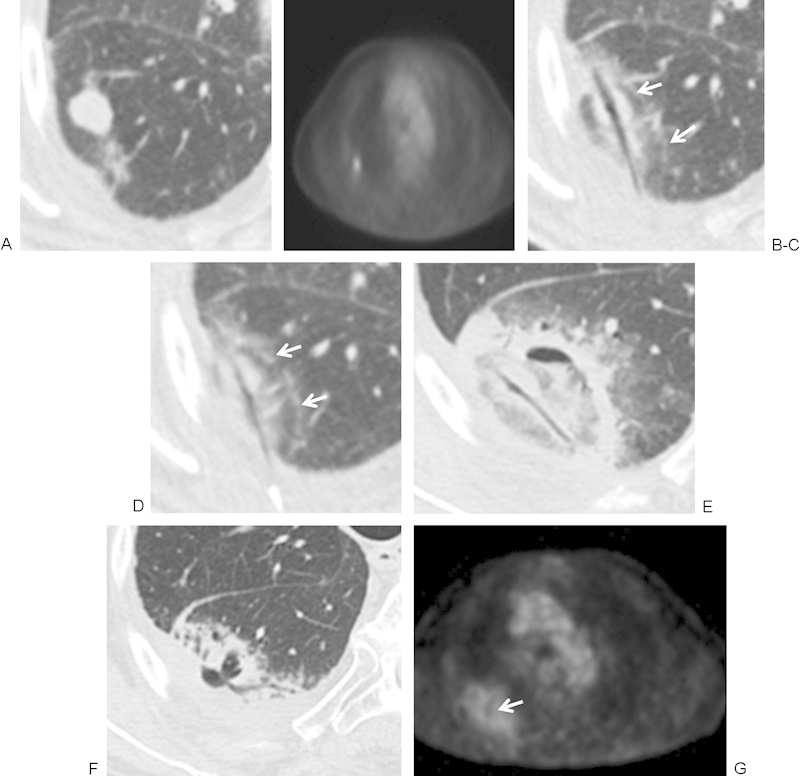
(A, B) Computed tomography (CT) and positron emission tomography (PET) images of a 77-year-old man with adenocarcinoma of the lung in the superior segment of the right lower lobe obtained 1 week before ablation demonstrates a hypermetabolic nodule. (C, D) Microwave ablation (MWA) was performed with the patient in the prone position using a posterior approach and using 45 W for 7 minutes. Images are rotated to maintain continuity of lesion location. Immediately after the ablation there is central tissue desiccation and cavitation along the antennae tract. A second layer and rim of faint ground-glass opacity (GGO) surrounds the tumor and represents tissue necrosis. An outermost rim of denser GGO (white arrows) represents congested lung tissue and hemorrhage that retains viability. (E) Approximately 48 hours after MWA, there is an area of cavitation in the postablation zone, and the antennae tract remains desiccated. The ablation zone is larger than the pretreatment tumor and represents hemorrhage, edema, and necrotic tissue. With time the ablation zone should regress in size. (F, G) CT and PET at 6 weeks postablation. There is a decrease in size of the postablation zone and surrounding hemorrhage, with persistent central cavitation. The PET activity has returned to mediastinal blood pool activity with a central area of absent uptake corresponding to cavitation (arrow).