
Figure 4.
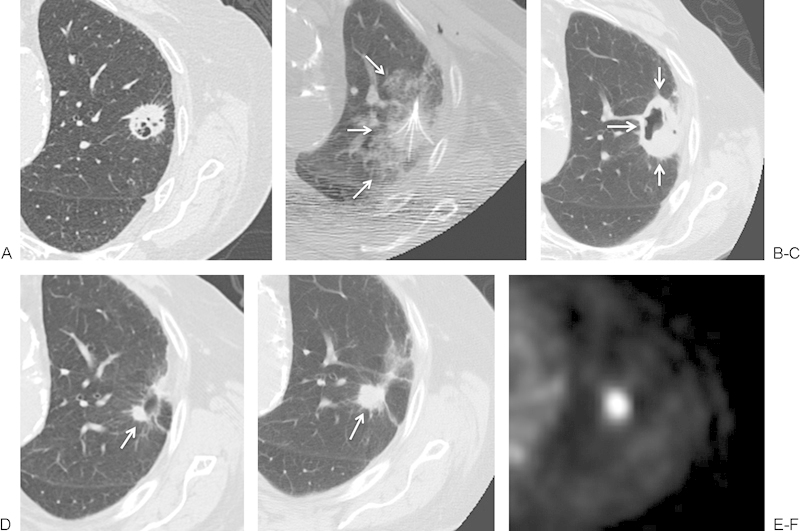
(A, B) An 84-year-old man with a biopsy-proven cavitary left upper lobe squamous cell carcinoma. Based on significant cardiovascular risk factors precluding surgical resection, the patient was referred for radiofrequency ablation. A multi-array electrode was used to perform overlapping ablations at 3 cm and 4 cm, each for 15 minutes. (B) The intra-ablation imaging demonstrated a rim of ground glass (white arrows) completely surrounding the mass. (C) At 5 weeks following treatment, the ablation zone (white arrows) consists of eccentric cavitation, covering the extent of the target lesion. (D) By 6 months, a nodule (white arrow) remains along the margin of the otherwise fully scarred ablation zone. (E, F) At 13 months, this nodule has grown (white arrow) and displays intense fluorodeoxyglucose uptake on positron emission tomography, compatible with residual tumor.