
Figure 1.
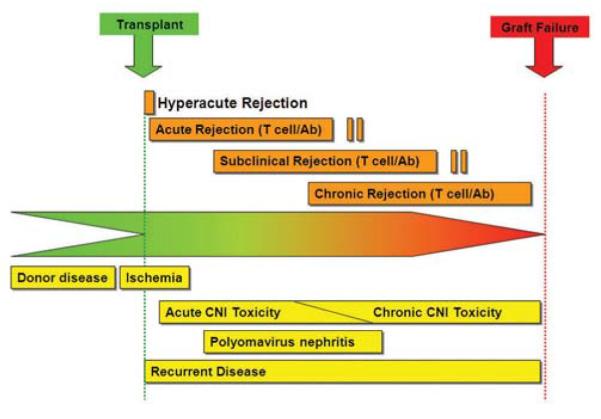
Timing of complications after kidney transplantation in allograft recipients. The differential diagnosis varies with the time since transplantation. Conditions above the line are related to immune rejection, and those below it to nonrejection causes of graft failure. Analysis of biopsy samples is needed to distinguish between these two categories of complications, which require different treatment. In the first few days after transplantation, the major concerns are post-transplantation acute tubular injury, anastomic complications of vessels and ureter with thrombosis, or obstruction, and hyperacute rejection. The following several weeks are dominated principally by acute antibody or cell-mediated rejection, acute drug toxicity, infection, occasionally recurrent disease, as well as lingering acute tubular injury and vascular complications. Up to 1 year post-transplantation, the issues include chronic drug toxicity, infection, recurrent disease, acute rejection, obstruction and renal artery stenosis. After the first year the major problems leading to graft dysfunction are chronic antibody-mediated rejection, chronic calcineurin inhibitor toxicity, recurrent glomerular disease and infection. Acute rejection can also occur at any time, particularly as a consequence of reduced immunosuppression (patient initiated or iatrogenic). *Rejection can be humoral or cell mediated. Abbreviation: CNI, calcineurin inhibitor. Permission obtained from Nature Publishing Group © Chapman et al. Kidney Int. Suppl. 99, S108–S112 (2005).