

Abstract
Multiple different surgical techniques have previously been described to address long head of the biceps tendinopathy. Subpectoral biceps tenodesis has proven to be an effective procedure to relieve pain and maintain function. We describe a surgical technique for subpectoral biceps tenodesis using a single double-loaded suture anchor implant. Advantages of this procedure include the ease of implant placement and the freedom this technique affords to perform the anchor placement without direct visualization of the docking site.
The biceps tenodesis procedure has been shown to be an effective surgical treatment for various symptomatic pathologic conditions related to the long head of the biceps brachii (LHB) tendon.1, 2, 3, 4, 5 By establishing a new fixed origin for the LHB attachment, the length-tension relation of the biceps muscle is maintained.6 Compared with LHB tenotomy, maintenance of this relation may preserve greater elbow flexion and forearm supination strength5 while also eliminating the risk of a “Popeye” deformity developing.7 Although surgical indications vary to some degree based on the treating surgeon's guidelines, general disease conditions that warrant consideration for biceps tenodesis include partial-thickness tears of the tendon greater than 25% to 50%, medial subluxation of the tendon with or without an associated subscapularis tear, chronic recalcitrant anterior shoulder pain attributed to LHB tendonitis, and pathology in association with certain SLAP tears and failed SLAP repairs.5
Multiple surgical options for LHB tenodesis have previously been reported, studied, and compared, with innumerable variations related to the tenodesis location (proximal v distal to bicipital groove), surgical approach (arthroscopic v open), and surgical implants used.1, 2, 3, 4, 5, 8, 9, 10, 11 In this article we describe and demonstrate a surgical technique for subpectoral biceps tenodesis using a single double-loaded Mitek Lupine suture anchor (DePuy Mitek, Raynham, MA) (Table 1, Video 1).
Table 1.
Summary of Main Steps and Associated Key Points to Complete Described Subpectoral Biceps Tenodesis Procedure
| Steps | Key Points |
|---|---|
| Arthroscopic biceps tenotomy | Perform intra-articular visualization of biceps tendon and superior labrum to assess need for biceps tenodesis procedure |
| Subpectoral incision with tendon isolation | Place 3- to 4-cm incision about anteromedial proximal humerus, with superior extent of incision at inferior border of pectoralis major, and locate tendon deep within wound |
| Anchor site preparation and placement | Perform anchor placement 1 cm proximal to inferior border of pectoralis major, in line with bicipital groove |
| Suture tendon and seat on anchor | Begin suturing 1 cm adjacent to musculotendinous junction, and travel toward cut tendon end with 3 locked suture passes on either side of tendon |
Surgical Technique
Although the operation can be successfully performed with the patient in the lateral decubitus position, we typically perform this procedure with the patient in the beach-chair position when the surgical plan includes a subpectoral biceps tenodesis, given the ease of surgical access afforded by this arrangement. A mechanical arm holder, such as the Spider Limb Positioner (Smith & Nephew, Memphis, TN), may be used, or an assistant can hold and position the arm for the procedure (Fig 1). A diagnostic arthroscopy is performed first, and all intra-articular pathology encountered is addressed. During this portion of the procedure, the LHB tendon, superior labrum, and surrounding structures (i.e., rotator cuff and cartilage surfaces) are evaluated and probed. For a more accurate inspection of the tendon, some authors advocate initially evaluating the intra-articular portion of the LHB tendon “dry,” to assess the tendon before the elevated pressures from joint insufflation compress and mask the inflamed vessels about the tendon sheath.3, 5
Fig 1.
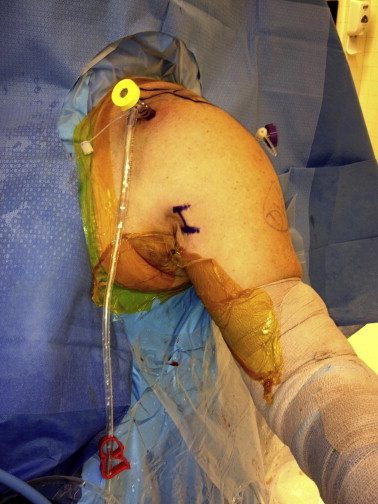
Standard beach-chair positioning for subpectoral biceps tenodesis. The patient's arm is typically abducted and externally rotated to allow access to the anteromedial proximal arm. The planned incision is marked.
The biceps tenotomy is performed with arthroscopic scissors introduced through the anterior portal. For efficiency purposes, care is taken to perform the tenotomy of the tendon directly at the superior labral insertion, so as to avoid leaving behind a tendon stump requiring additional debridement. Before completion of the tenotomy, the tendon can be tagged with a No. 1 polydioxanone (PDS) suture (Ethicon, Somerville, NJ) passed through a spinal needle, but this is not required5 and not typically performed at our institution. The subpectoral approach and tenodesis are often performed next, before moving to the subacromial space, because the shoulder tissue edema from prolonged subacromial fluid extravasation can make locating the tendon and performing the tenodesis more difficult.
For the subpectoral approach, the arm positioner is adjusted to place the shoulder in 20° to 30° of abduction and 30° of external rotation. An approximately 2- to 3-cm incision is made about the anteromedial aspect of the proximal humerus, adjacent to the axilla and beginning approximately 1 cm superior to the palpable pectoralis major tendon5 (Fig 1). The dissection is directed toward the humerus, avoiding the medially based neurovascular structures. The biceps tendon will be palpable deep to the investing fascia over the biceps and coracobrachialis, traveling superiorly into the bicipital groove and deep to the pectoralis major tendon. Blunt dissection straight to the humerus, beneath the pectoralis major tendon, will consistently lead the surgeon to the tendon and help avoid errant dissection.5
Once located, the tendon is then delivered into the wound with either the surgeon's finger or a right-angle clamp. An Alice clamp is then applied to the cut proximal tendon end, and attention is directed to preparing the humerus for anchor placement. The ideal location for the anchor is approximately 1 cm proximal to the distal extent of the pectoralis major tendon, in line with the bicipital groove.5 This location can be blindly palpated through a small incision. The instruments required for the procedure are then assembled and include a Mitek 2.9-mm drill bit and drill guide (DePuy Mitek), a rasp (any variety), and the Mitek Lupine anchor on a metal inserter (Fig 2). A power drill and a small mallet are also needed. The anchor site is first rasped to prepare the cortical bed. By placing one's index finger on the instrument end of the rasp while holding the handle with the rest of the hand, excellent precision control of the rasp is obtainable, which allows the selected anchor position to be located blindly once again (Video 1).
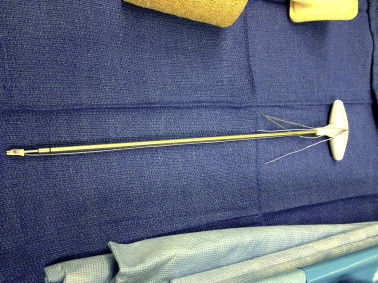
Fig 2.

Instruments required for our procedure include (from left to right) the Mitek drill guide, the Mitek 2.9-mm drill, and a rasp for preparing the docking site.
Next, the drill guide for the Mitek 2.9-mm drill bit is positioned on this same location (Fig 3). A unicortical drill hole is created and the drill removed while the drill guide is maintained in the same position (Fig 4). One safety feature of this system is that the Mitek 2.9-mm drill bit and drill guide are designed so that the drill “bottoms out” and does not advance further after the first cortex is breached. The Lupine anchor, on the insertion handle (Fig 5), is then passed through the guide to introduce the implant into the cortical drill hole (Fig 6). Full insertion of the implant typically requires a few gentle mallet strikes. Once seated, the inserter is then disengaged from the implant with 9 to 10 counterclockwise turns after disengaging the suture from the back end of the inserter. Once the drill guide and inserter have been removed from the wound, the anchor is seated within the intramedullary canal with a gentle tug (8 lb of pressure is recommended) on the sutures (Video 1).
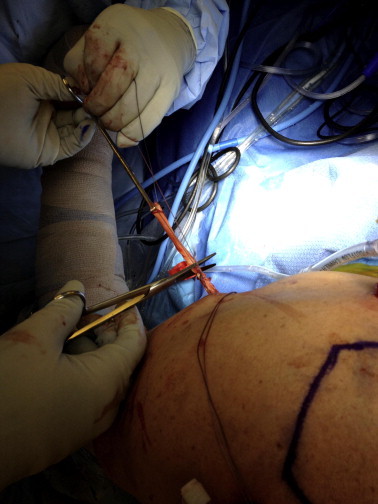
Fig 3.

Blindly positioning drill guide in line with bicipital groove, 1 cm proximal to inferior border of pectoralis major muscle.
Fig 4.

Drilling unicortical hole for anchor placement. The drill guide position is maintained after the drill is removed for ease of anchor placement.
Fig 5.
Double-loaded Lupine anchor on metal inserter handle.
Fig 6.

Placement of Lupine anchor through drill guide.
Because the implant is double loaded, 4 suture strands—2 violet and 2 blue—of equal length will be exiting the wound. By use of a free curved suture needle, 1 blue strand is sutured to the tendon, beginning 1 cm adjacent to the musculotendinous junction and continuing toward the cut tendon end. Three to four locked Krackow-type passes are made traveling longitudinally down 1 side of the tendon (Fig 7). The same technique is then performed along the other side of the tendon with 1 of the violet suture strands. The excess tendon proximal to the last suture passes is then cut (Fig 8). Care should be taken to make these locked suture passes close together longitudinally to avoid subsequent bunching of the tendon. The free blue and violet suture strands then become the posts, and pulling tension on these 2 sutures will shuttle the tendon down to the anchor (Fig 9). Maintaining tension on both “posts,” the sutured violet strand is then tied freehand to the violet post, followed by tying of the blue sutures in the same manner, completing the tenodesis (Fig 10).
Fig 7.

Suturing of proximal aspect of biceps tendon.
Fig 8.
Excision of excess proximal tendon.
Fig 9.

Shuttling tendon into position by pulling on 2 suture posts.
Fig 10.
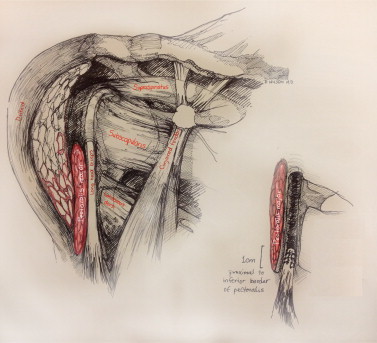
Artistic rendition of our subpectoral biceps tenodesis technique, with surrounding anatomic structures highlighted.
The wound is then irrigated and closed in a layered fashion. Postoperative rehabilitation, excluding changes made for additional procedures, typically entails 2 weeks of sling immobilization, progression to gentle active glenohumeral and elbow range of motion by 4 weeks, and avoidance of resisted elbow flexion and supination for 6 to 8 weeks.
Discussion
Although the LHB tenodesis location and technique continue to be debated, purported advantages of the open subpectoral procedure include ease of technique and elimination of residual “groove pain” while still maintaining an adequate length-tension relation.5 Prior publications have advocated performing the tenodesis 1 cm proximal to the musculotendinous junction to a location 1 cm proximal to the distal extent of the pectoralis major on the humerus,3, 5 which has recently been reaffirmed by cadaveric research.6 Biomechanical studies suggest that biotenodesis screws provide stronger fixation compared with suture anchors in cadaveric models,8, 9, 10 but in vivo studies have not shown a clinical difference in implant types4 and failures of the biotenodesis screw have been reported.11, 12
The Mitek Lupine anchor is an absorbable implant composed of poly(lactide-coglycolide) polymer and tricalcium phosphate. Docked on a stainless steel inserter, the anchor is double loaded with two No. 2 Orthocord sutures (DePuy Mitek) (1 blue and 1 violet) through a sliding eyelet. Previous reports have been published exploring the use of this implant for SLAP and Bankart repairs,13, 14 but a subpectoral biceps tenodesis technique using the Lupine anchor has not been previously published.
A significant advantage of the described technique is the ability it affords to perform the entirety of the procedure “blind” with palpation of the tenodesis site only. Nearly all previously described techniques, involving drill holes, biotenodesis screws, and other manufacturers' suture anchors, recommend direct visualization of the drill hole(s) for the fixation portion of the procedures.1, 2, 3, 4, 5 This requires broader exposure with multiple retractors, with the associated risk of neurovascular compression, and a knowledgeable assistant to hold retraction. With the previously described technique, the incision only needs to be wide enough to locate and extract the tendon, and retractors and assistants are not needed. The drill hole does not need to be “found” within the wound, because the drill guide holds the position while the implant is inserted.
The majority of the risks associated with our technique are shared by all biceps tenodesis procedures. While the surgeon is isolating the tendon within the subpectoral wound, care must be taken to avoid errantly dissecting too far medially, which could lead to iatrogenic neurovascular injury. Proximal humeral fracture after “keyhole” biceps tenodesis procedures has also been described.15, 16 In our experience, wound complications and infection at this surgical site are extremely rare.
Over 200 subpectoral biceps tenodesis procedures have been performed at our institution using the described technique over the last 4 years, without any known failures to date. This procedure has proven to be an efficient, reproducible, and reliable means of treating LHB tendon pathology commonly seen in our active military population.
Acknowledgment
The authors thank Julian Arroyo, M.D. for his contributions to the development of this surgical technique.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article. The views expressed are those of the authors and do not reflect the official policy of the Department of the Army, the Department of Defense, or the US Government.
Supplementary Data
Brief surgical demonstration of our technique.
References
- 1.Boileau P., Krishnan S.G., Coste J.S., Walch G. Arthroscopic biceps tenodesis: A new technique using bioabsorbable interference screw fixation. Arthroscopy. 2002;18:1002–1012. doi: 10.1053/jars.2002.36488. [DOI] [PubMed] [Google Scholar]
- 2.Mazzocca A.D., Romeo A.A. Arthroscopic biceps tenodesis in the beach chair position. Oper Tech Sports Med. 2003;11:6–14. [Google Scholar]
- 3.Mazzocca A.D., Rios C.G., Romeo A.A., Arciero R.A. Subpectoral biceps tenodesis with interference screw fixation. Arthroscopy. 2005;21:896e1–896e7. doi: 10.1016/j.arthro.2005.04.002. [DOI] [PubMed] [Google Scholar]
- 4.Millett P.J., Sanders B., Gobezie R., Braun S., Warner J.P. Interference screw vs. suture anchor fixation for open subpectoral biceps tenodesis: Does it matter? BMC Musculoskelet Disord. 2008;9:121. doi: 10.1186/1471-2474-9-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Provencher M.T., LeClere L.E., Romeo A.A. Subpectoral biceps tenodesis. Sports Med Arthrosc Rev. 2008;16:170–176. doi: 10.1097/JSA.0b013e3181824edf. [DOI] [PubMed] [Google Scholar]
- 6.Denard P.J., Dai X., Hanypsiak B.T., Burkhart S.S. Anatomy of the biceps tendon: Implications for restoring physiological length-tension relation during biceps tenodesis with interference screw fixation. Arthroscopy. 2012;28:1352–1358. doi: 10.1016/j.arthro.2012.04.143. [DOI] [PubMed] [Google Scholar]
- 7.Wolf R.S., Zheng N., Weichel D. Long head biceps tenotomy versus tenodesis: A cadaveric biomechanical analysis. Arthroscopy. 2005;21:182–185. doi: 10.1016/j.arthro.2004.10.014. [DOI] [PubMed] [Google Scholar]
- 8.Mazzocca A.D., Bicos J., Santangelo S., Romeo A.A., Arciero R.A. The biomechanical evaluation of four fixation techniques for proximal biceps tenodesis. Arthroscopy. 2005;21:1296–1306. doi: 10.1016/j.arthro.2005.08.008. [DOI] [PubMed] [Google Scholar]
- 9.Ozalay M., Akpinar S., Karaeminogullari O. Mechanical strength of four different biceps tenodesis techniques. Arthroscopy. 2005;21:992–998. doi: 10.1016/j.arthro.2005.05.002. [DOI] [PubMed] [Google Scholar]
- 10.Golish S.R., Caldwell P.E., Miller M.D. Interference screw versus suture anchor fixation for subpectoral tenodesis of the proximal biceps tendon: A cadaveric study. Arthroscopy. 2008;24:1103–1108. doi: 10.1016/j.arthro.2008.05.005. [DOI] [PubMed] [Google Scholar]
- 11.Nho S.J., Reiff S.N., Verma N.N., Slabaugh M.A., Mazzocca A.D., Romeo A.A. Complications associated with subpectoral biceps tenodesis: Low rates of incidence following surgery. J Shoulder Elbow Surg. 2010;19:764–768. doi: 10.1016/j.jse.2010.01.024. [DOI] [PubMed] [Google Scholar]
- 12.Koch B.S., Burks R.T. Failure of biceps tenodesis with interference screw fixation. Arthroscopy. 2012;28:735–740. doi: 10.1016/j.arthro.2012.02.019. [DOI] [PubMed] [Google Scholar]
- 13.Barber F.A., Coons D.A., Ruiz-Suarez M. Cyclic load testing and ultimate failure strength of biodegradable glenoid anchors. Arthroscopy. 2008;24:224–228. doi: 10.1016/j.arthro.2007.08.011. [DOI] [PubMed] [Google Scholar]
- 14.Sileo M.J., Lee S.J., Kremenic I.J. Biomechanical comparison of a knotless suture anchor with standard suture anchor in the repair of type II SLAP tears. Arthroscopy. 2009;25:348–354. doi: 10.1016/j.arthro.2008.10.019. [DOI] [PubMed] [Google Scholar]
- 15.Reiff S.N., Nho S.J., Romeo A.A. Proximal humerus fracture after keyhole biceps tenodesis. Am J Orthop. 2010;39:E61–E63. [PubMed] [Google Scholar]
- 16.Friedel R., Markgraf E., Schmidt I., Donicke T. Proximal humerus shaft fracture as a complication after keyhole-plasty: A case report. Unfallchirurgie. 1995;21:198–201. doi: 10.1007/BF02588699. (in German) [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Brief surgical demonstration of our technique.