

Abstract
Purpose
This study was to determine the prevalence of herniated intervertebral disc (HIVD) among Korean 19-year-old male in a large national sample and to compare the prevalence across geographic regions based on the data of conscription.
Materials and Methods
We analyzed the conscription data of 615508 cases who were 19-year-old male, given an examination for conscription at nationwide Korean Military Manpower Administration from January 2008 to December 2009. Prevalence was determined by dividing the number of cases by the number of persons enrolled for 2 years. The analyses included of a cross-tabulations and nonparametric chi-square to compare the prevalence according to geographic region, disc severity, and conscription year.
Results
The prevalence of HIVD among 19-year-old male was 0.47%. Seoul had the highest prevalence of HIVD (total HIVD was 0.60%, and severe HIVD was 0.44%). The prevalence of HIVD was lower in Jeollabuk-do and Jeollanam-do (total HIVD was 0.25-0.27%, and severe HIVD was 0.16-0.17%). Annual prevalence of HIVD was slightly decreased in 2009, but geographic distribution annually was not different.
Conclusion
In Korean 19-year-old male, the national prevalence of adolescent HIVD was 0.60%, but different geographic distribution was observed. It is quite possible that secondary contributing factor(s) interfere with the different geographic prevalence of HIVD.
Keywords: Herniated intervertebral disc, adolescent, prevalence, conscription
INTRODUCTION
The rate of prevalence is the number of people in a population who has a disease for a given amount of time. The numerator is the number of existing cases of disease at a specified time, and the denominator is the total population. The interference of prevalence is not well known, and the interference of spinal disease prevalence remains also obscure. Intervertebral disc herniation (HIVD) is a common disorder, but precise frequency of this condition is not clearly defined. Geographic distribution is also not well known. This study was to determine the prevalence of HIVD among Korean 19-year-old male in a large national sample and to compare the prevalence across geographic regions based on the data of conscription.
MATERIALS AND METHODS
Since Korea has adopted the conscription system and all men are examined for conscription at the Military Manpower Administration (MMA) when they are 19-year-old. This cross-sectional survey was conducted by the analysis of the conscription data of all Korean regional MMA from January 2008 to December 2009. During this period, total 615508 Korean 19-year-old males participated in the conscription, and this case number covered more than 99% of the Korean 19-year-old male population.
The conscription data were reviewed according to the disc severity. HIVD was classified into 5 groups of disc severity according to the law of Korean military affairs, and the categories are shown in Table 1. The severity of HIVD was defined by using spine MRI. However, it is impossible to take spine MRI for all the candidates due to economical reason and limited time. Therefore, MRI was taken only in those who have taken MRI personally and candidates who have symptoms, uncovered by surveys and interviews.
Table 1.
Categories Classifying Herniated Intervertebral Disc According to the Law of Korean Military Affairs

MMA, Military Manpower Administration.
*Positive result of electromyogram test was defined as matched radiculopathy finding according to suspicious level of herniation.
†Spinal canal stenosis was defined as the narrowing of the spinal canal more than 50% of mid-sagittal diameter (front to back) in the same plane of imaging study.
‡Cut-off sign was defined as all loss of signal in neuromuscular at the interesting level using imaging study.
In the schematic review about HIVD, HIVD without thecal sac compression was considered as moderate severity, and HIVD with thecal sac compression was considered as severe severity. The presence of simple discectomy or spinal procedure was not considered, and the preoperative herniation severity was considered to confirm the disc severity. The spinal fusion cases by HIVD were excluded from the study, although the cases were very few.
The national prevalence of HIVD was calculated by total HIVD cases and total conscription examinees. The geographic distribution was conducted according to the jurisdiction of regional MMA. Regional MMA was located in 12 locations, as shown in Fig. 1: Seoul, Northern Gyeonggi-do, Southern Gyeonggi-do, Kangwon-do, Chungcheongbuk-do, Chungcheongnam-do, Gyeongsangbuk-do, Gyeongsangnam-do, Jeollabuk-do, Jeollanam-do, Busan, and Jeju-do.
Fig. 1.

The geographic illustration of the jurisdiction of regional Military Manpower Administration in the Republic of Korea. SU, Seoul; GGB, Northern Gyeonggi-do; GGN, Southern Gyeonggi-do; KWD, Kangwon-do; CCB, Chungcheongbuk-do; CCN, Chungcheongnam-do; GSB, Gyeongsangbuk-do; GSN, Gyeongsangnam-do; JLB, Jeollabuk-do; JLN, Jeollanam-do; BS, Busan; JJD, Jeju-do.
The geographic distribution of HIVD was also annually reviewed to check observational bias. The disease of HIVD was conducted at the neurosurgery department in Korean MMA, and neurosurgeons and radiologists consisted of 16 members each while annually changing the place of work. Therefore, the authors could estimate the presence of bias by checking the difference of a regional HIVD proportion.
The analyses were composed of a cross-tabulations and nonparametric chi-square to compare prevalence by geographic region, disc severity, and conscription year. Tests were considered significant at p-values less than 0.01, because of the large number of cases. This study was conducted with an approval of the committee in the MMA in Seoul.
RESULTS
National prevalence of HIVD among Korean 19-year-old males is shown in Table 2. Among 615508 Korean 19-year-old male examinees for conscription, 2905 cases were diagnosed as HIVD, and the nationwide prevalence of HIVD was 0.47%. The nationwide prevalence of severe HIVD was 0.32%.
Table 2.
Demografic Distribution of Herniated Intervertebral Disc According to Disc Severity in 19-Year-Old Males in the Republic of Korea from 2008 to 2009
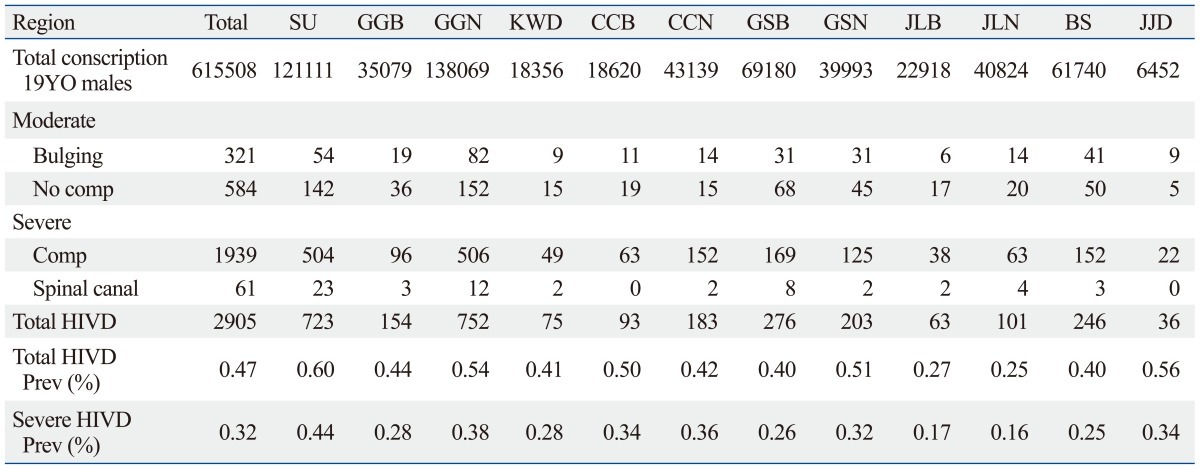
SU, Seoul; GGB, Northern Gyeonggi-do; GGN, Southern Gyeonggi-do; KWD, Kangwon-do; CCB, Chungcheongbuk-do; CCN, Chungcheongnam-do; GSB, Gyeongsangbuk-do; GSN, Gyeongsangnam-do; JLB, Jeollabuk-do; JLN, Jeollanam-do; BS, Busan; JJD, Jeju-do; HIVD, herniated intervertebral disc.
Geographic prevalence of HIVD among the examinees is shown in Table 2 and Fig. 2. The highest prevalence of HIVD was found in Seoul. In Seoul, the prevalence of total HIVD and severe HIVD was 0.60% and 0.44%, respectively. The 2nd and 3rd highest prevalence of total HIVD appeared in Jeju-do (0.56%) and Southern Gyeonggi-do (0.54%). The 2nd and 3rd highest prevalence of severe HIVD was found in Southern Gyeonggi-do (0.36%) and Jeju-do (0.34%). The low prevalence of HIVD was observed in Jeollabuk-do and Jeollanam-do. The prevalence of total HIVD was 0.25-0.27%, and the prevalence of severe HIVD was 0.16-0.17% in these regions.
Fig. 2.

National and geographic prevalence of total HIVD and severe HIVD among Korean 19-year-old males. SU, Seoul; GGB, Northern Gyeonggi-do; GGN, Southern Gyeonggi-do; KWD, Kangwon-do; CCB, Chungcheongbuk-do; CCN, Chungcheongnam-do; GSB, Gyeongsangbuk-do; GSN, Gyeongsangnam-do; JLB, Jeollabuk-do; JLN, Jeollanam-do; BS, Busan; JJD, Jeju-do; HIVD, herniated intervertebral disc.
The statistical differences of the geographical prevalence are shown in Table 3. The bright and dark gray cells indicate the difference of total and severe HIVD among two regions, respectively. In Table 3, the statistical differences were found mostly in the comparision of Seoul, Jeollabuk-do, and Jeollanam-do (p-value <0.001).
Table 3.
The Statistical Differences in Geographical Prevalence between Two Regions
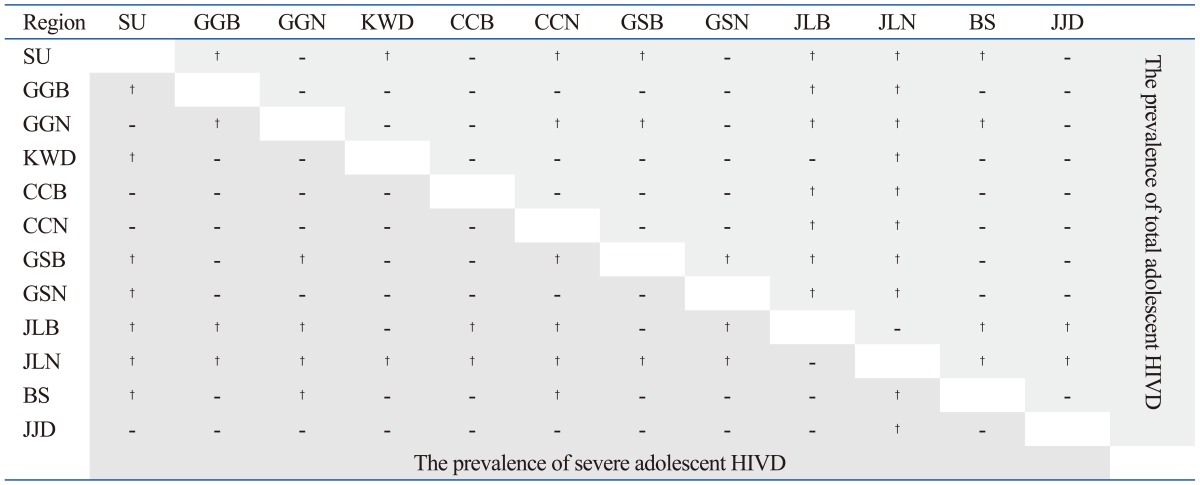
SU, Seoul; GGB, Northern Gyeonggi-do; GGN, Southern Gyeonggi-do; KWD, Kangwon-do; CCB, Chungcheongbuk-do; CCN, Chungcheongnam-do; GSB, Gyeongsangbuk-do; GSN, Gyeongsangnam-do; JLB, Jeollabuk-do; JLN, Jeollanam-do; BS, Busan; JJD, Jeju-do; HIVD, herniated intervertebral disc.
†Statistically differented with p-value lesser than 0.001.
The analysis of annual prevalence of HIVD, demonstrated that the prevalence of total HIVD was significantly decreased in 2009 compared with 2008 (Table 4). The annual prevalence difference in total HIVD between 2008 and 2009 was only 0.002%. The annual prevalence difference of severe HIVD was also decreased in 2008 and 2009, but statistical difference was not satisfactory (p<0.025). Furthermore, the prevalence of total HIVD only in Southern Gyeonggi-do decreased significantly in 2009 compared with 2008, and other regions did not show statistical differences.
Table 4.
The Annual Geographical Prevalence of Total HIVD and Severe HIVD among Korean 19-Year-Old Males in 2008 and 2009

SU, Seoul; GGB, Northern Gyeonggi-do; GGN, Southern Gyeonggi-do; KWD, Kangwon-do; CCB, Chungcheongbuk-do; CCN, Chungcheongnam-do; GSB, Gyeongsangbuk-do; GSN, Gyeongsangnam-do; JLB, Jeollabuk-do; JLN, Jeollanam-do; BS, Busan; JJD, Jeju-do; HIVD, herniated intervertebral disc.
DISCUSSION
In the prevalence study, pediatric patients constitute roughly 0.5-6.8% of all patients hospitalized for HIVD.1-9 The first report of a HIVD in a child was published in 1934, and the first report of surgical treatment in a child (a 12-year-old boy) was issued in 1945. In the literature review, there was a prevalence study about Korean adolescent HIVD.5 This study was based on examination of Korean conscription, and reported that the prevalence of HIVD in adolescent, aged 19 years old and younger, was 0.5% (382 cases among 77685 examinees).
The precise prevalence of adolescent HIVD still remains controversy. The actual incidence of adolescent HIVD is difficult to establish due to the following reasons. First, published series adopted different ranges of age.4,7,10,11 When an upper limit of 15 years was adopted, an epidemiologic study, following 12058 Finnish babies from birth until 28 years of age, showed no prevalence of confirmed HIVD. However, significantly increased number of cases (0.1-0.2%) were found with the upper limit of 20 years old.12 By the age of 28 years, 9.5% of males and 4.2% of females were admitted to hospitals with a diagnosis of HIVD, respectively.
Another reason is that real cause of HIVD in adolescents still requires explanation. Several factors have been investigated, such as trauma, congenital malformations, growth disturbances, familial predisposition, the presence of morphologic and functional alterations, and vertebral slipping epiphysis. Trauma, which is considered to be a severe physical stress on the lumbo-sacral spine, is often regarded as a reasonable factor.2 One of the most likely factors expounding the early onset of HIVD is the relation with vertebral deformities, such as scoliosis, transitional defects, schisis, and canal narrowing. A feature that characterizes HIVD in adolescents is difficult to evaluate subjective symptoms, and clinical signs could be one of reasons. Clinical presentations of adolescent HIVD are generally similar to those of adults. However, up to 90% of adolescent patients have a positive straight-leg raise test2,13 which differentiates adolescent and adult HIVD, because children and adolescents tend to have greater nerve root tension than adults.14 Furthermore, this is often accompanied by neurological symptoms, such as, numbness and weakness.15-17 Therefore, the time interval between the onset of symptoms and diagnosis is generally very long, averaging 6 months in the current series.18
In this study, the incidence of adolescent HIVD was 0.60% in Korean 19-year-old males. This result is very similar to a recent study. Presently, there are several studies on the prevalence of adolescent HIVD, but 'real' prevalence has been hard to determine because of the reasons explained above. Our investigation was limited to only 19-year-old male, however, data covered more than 99% of population (census data) by using the governmental military conscription data, therefore, this study is less likely affected by sampling survey bias. As a result, this investigation could be more superior and accurate than other prevalence studies. Furthermore, this is the first report on the prevalence by regional differences in Korea: in these geographic results, significant differences were observed by some regions. However, it is not clear why differences are seen among the regions; the reasons for the differences could be social economic status, motivation for hospitalization, trauma rate, number of hospitals and etc. Since, there is no study on the relationship between HIVD and the above factors, further evaluation is necessary. Finally, there is a limitation in the fact that all the files of follow-up results and treatment of diagnosed diseases do not exist for the purpose of conscription in military service.
In conclusion, in Korean 19-year-old males, the prevalence of adolescent HIVD was 0.60%, and severe adolescent HIVD was relatively highly prevalent (0.28%). The MMA physical grade was useful to conscription as they represent disability by HIVD.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Borgesen SE, Vang PS. Herniation of the lumbar intervertebral disk in children and adolescents. Acta Orthop Scand. 1974;45:540–549. doi: 10.3109/17453677408989177. [DOI] [PubMed] [Google Scholar]
- 2.Epstein JA, Epstein NE, Marc J, Rosenthal AD, Lavine LS. Lumbar intervertebral disk herniation in teenage children: recognition and management of associated anomalies. Spine (Phila Pa 1976) 1984;9:427–432. doi: 10.1097/00007632-198405000-00019. [DOI] [PubMed] [Google Scholar]
- 3.Epstein JA, Lavine LS. Herniated lumbar intervertebral discs in teen-age children. J Neurosurg. 1964;21:1070–1075. doi: 10.3171/jns.1964.21.12.1070. [DOI] [PubMed] [Google Scholar]
- 4.Hashimoto K, Fujita K, Kojimoto H, Shimomura Y. Lumbar disc herniation in children. J Pediatr Orthop. 1990;10:394–396. doi: 10.1097/01241398-199005000-00019. [DOI] [PubMed] [Google Scholar]
- 5.Heithoff KB, Gundry CR, Burton CV, Winter RB. Juvenile discogenic disease. Spine (Phila Pa 1976) 1994;19:335–340. doi: 10.1097/00007632-199402000-00014. [DOI] [PubMed] [Google Scholar]
- 6.Kurihara A, Kataoka O. Lumbar disc herniation in children and adolescents. A review of 70 operated cases and their minimum 5-year follow-up studies. Spine (Phila Pa 1976) 1980;5:443–451. [PubMed] [Google Scholar]
- 7.Matsui H, Terahata N, Tsuji H, Hirano N, Naruse Y. Familial predisposition and clustering for juvenile lumbar disc herniation. Spine (Phila Pa 1976) 1992;17:1323–1328. doi: 10.1097/00007632-199211000-00011. [DOI] [PubMed] [Google Scholar]
- 8.Pietilä TA, Stendel R, Kombos T, Ramsbacher J, Schulte T, Brock M. Lumbar disc herniation in patients up to 25 years of age. Neurol Med Chir (Tokyo) 2001;41:340–344. doi: 10.2176/nmc.41.340. [DOI] [PubMed] [Google Scholar]
- 9.Wahren H. Herniated nucleus pulposus in a child of twelve years. Acta Orthop Scand. 1945;16:40–42. doi: 10.3109/17453674508988913. [DOI] [PubMed] [Google Scholar]
- 10.Callahan DJ, Pack LL, Bream RC, Hensinger RN. Intervertebral disc impingement syndrome in a child. Report of a case and suggested pathology. Spine (Phila Pa 1976) 1986;11:402–404. doi: 10.1097/00007632-198605000-00021. [DOI] [PubMed] [Google Scholar]
- 11.Luukkonen M, Partanen K, Vapalahti M. Lumbar disc herniations in children: a long-term clinical and magnetic resonance imaging follow-up study. Br J Neurosurg. 1997;11:280–285. doi: 10.1080/02688699746041. [DOI] [PubMed] [Google Scholar]
- 12.Zitting P, Rantakallio P, Vanharanta H. Cumulative incidence of lumbar disc diseases leading to hospitalization up to the age of 28 years. Spine (Phila Pa 1976) 1998;23:2337–2343. doi: 10.1097/00007632-199811010-00017. [DOI] [PubMed] [Google Scholar]
- 13.Gennuso R, Humphreys RP, Hoffman HJ, Hendrick EB, Drake JM. Lumbar intervertebral disc disease in the pediatric population. Pediatr Neurosurg. 1992;18:282–286. doi: 10.1159/000120676. [DOI] [PubMed] [Google Scholar]
- 14.Matsui H, Kitagawa H, Kawaguchi Y, Tsuji H. Physiologic changes of nerve root during posterior lumbar discectomy. Spine (Phila Pa 1976) 1995;20:654–659. doi: 10.1097/00007632-199503150-00004. [DOI] [PubMed] [Google Scholar]
- 15.Clarke NM, Cleak DK. Intervertebral lumbar disc prolapse in children and adolescents. J Pediatr Orthop. 1983;3:202–206. doi: 10.1097/01241398-198305000-00009. [DOI] [PubMed] [Google Scholar]
- 16.Garrido E, Humphreys RP, Hendrick EB, Hoffman HJ. Lumbar disc disease in children. Neurosurgery. 1978;2:22–26. doi: 10.1227/00006123-197801000-00004. [DOI] [PubMed] [Google Scholar]
- 17.Ozgen S, Konya D, Toktas OZ, Dagcinar A, Ozek MM. Lumbar disc herniation in adolescence. Pediatr Neurosurg. 2007;43:77–81. doi: 10.1159/000098377. [DOI] [PubMed] [Google Scholar]
- 18.DeOrio JK, Bianco AJ., Jr Lumbar disc excision in children and adolescents. J Bone Joint Surg Am. 1982;64:991–996. [PubMed] [Google Scholar]