
Figure 5.
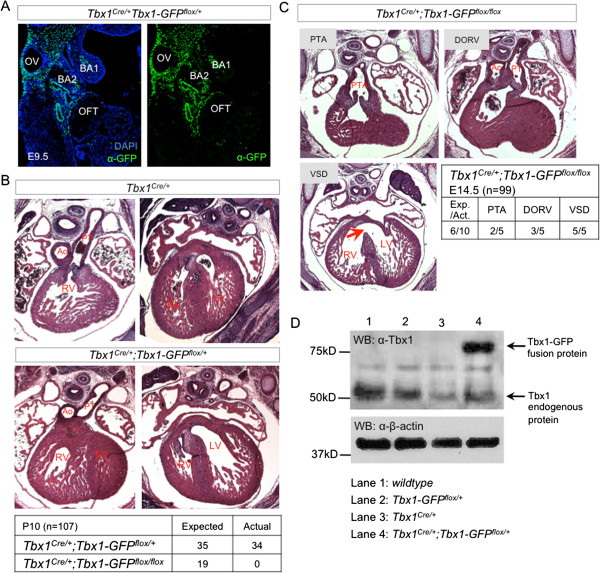
Dosage effects of Tbx1-GFP activation on heart development. (A) Immunofluorescence with a GFP antibody shows activation of Tbx1-GFP by Tbx1Cre/+ at E9.5. GFP is detected in the posterior otic vesicle (OV), 1st and 2nd branchial arches (BA1, BA2), and mesoderm including the secondary heart field proximal to the outflow tract (OFT). (B) Histological transverse sections at E14.5 shows that Tbx1Cre/+;Tbx1-GFPflox/+ mutants do not have outflow tract or ventricular defects. They survive in normal mendelian ratios, unlike Tbx1Cre/+;Tbx1-GFPflox/flox mutants which are not viable. (C) Activation of both alleles of Tbx1-GFP by Tbx1Cre/+ causes outflow tract septation (persistant truncus arteriosis, PTA) and alignment (double outlet right ventricle , DORV) defects with ventricular septal defect (VSD). (D) Western blot of proteins isolated from E9.5 pharyngeal regions to compare protein expression levels of Tbx1-GFP and endogenous Tbx1. For each genotype, we pooled 4 embryos (23–24 somite stage) and loaded equal amounts of protein per lane. The same membrane was probed with antibodies to Tbx1 and β-actin. The expected size of endogenous Tbx1 is ≈50 kD while the Tbx1-GFP fusion protein is ≈75kD. β-actin is detected at ≈40 kD.