

Abstract
The challenges for scholars committed to successful careers in clinical and translational science are increasingly well recognized. The Education and Career Development (EdCD) of the national Clinical and Translational Science Award consortium gathered thought leaders to propose sustainable solutions and an agenda for future studies that would strengthen the infrastructure across the spectrum of pre‐ and postdoctoral, MD and PhD, scholars. Six consensus statements were prepared that include: (1) the requirement for career development of a qualitatively different investigator; (2) the implications of interdisciplinary science for career advancement including institutional promotion and tenure actions that were developed for discipline‐specific accomplishments; (3) the need for long‐term commitment of institutions to scholars; (4) discipline‐specific curricula are still required but curricula designed to promote team work and interdisciplinary training will promote innovation; (5) PhD trainees have many pathways to career satisfaction and success; and (6) a centralized infrastructure to enhance and reward mentoring is required. Several themes cut across all of the recommendations including team science, innovation, and sustained institutional commitment. Implied themes include an effective and diverse job force and the requirement for a well‐crafted public policy that supports continued investments in science education. Clin Trans Sci 2012; Volume #: 1–6
Keywords: Clinical and Translational Science Award (CTSA), Education and Career Development (EdCD) key function committee, interdisciplinary, competencies, mentoring
Introduction
The nature of science, learned and practiced, is changing. Current research efforts have greater emphasis on interdisciplinary and team‐based approaches. 1 , 2 In addressing current public health challenges such as obesity, cancer, and mental health disorders, it is inconceivable that a single researcher, working alone, will make significant headway, particularly when one considers the need to transcend the continuum of research from basic discovery to social policy. For example, the National Center on Minority Health and Health Disparities consensus conference rejected incremental elimination of health inequities in favor of paradigmatic change based upon interdisciplinary, transformative translational research. 3 These challenges must be addressed by more comprehensive, multitiered strategies that engage well‐trained individuals from multiple disciplines. 4 Investigators must be prepared to lead and be effective members of dynamic matrices that solve these problems.
With the goal of improving the strategic career development of clinical translational scholars, and to produce an agenda for future studies, curricula development, and institutional policies, the Clinical and Translational Science Award (CTSA) Education and Career Development (EdCD) key function committee gathered information using special meetings, supplemental grants, working groups, white papers, and intercommittee collaboration to develop consensus statements ( Table 1 ).
Table 1.
Recommendations for the improvement of the career development of clinical and translational scholars.
| Clinical translational research requires the career development of a qualitatively different investigator. |
| Promotion and tenure requirements should reflect the emerging value on team science and mentoring. |
| The trajectory of training includes a long‐term commitment by institutions. |
| Discipline‐specific training is still required but curricula designed to promote teamwork and interdisciplinary training will promote innovation. |
| Ph.D. trainees can take advantage of multiple pathways to have a successful and satisfying career. |
| Mentoring requires a centralized infrastructure and rewards will promote excellence. |
Consensus Statement I
Clinical translational research requires the career development of a qualitatively different investigator
Individual challenges and opportunities for early career scientists involved in team science include the need for the multicultural, multilingual investigator as the cohesive force in complex investigations. 5 Complementary systemic changes are needed to support a shift in the trajectory of the junior investigator’s career development and discovery and implementation of the products of collaboration. Institutional competencies will be essential if career development programs, designed to support team science and effective research strategies, are developed to confront complex health problems.
Team‐based efforts are growing. In a 2004 study of more than 14,000 manuscripts published by four major medical journals, the average number of authors per paper rose from 4.5 in 1980 to 6.9 in 2000. 6 A similar analysis 7 led its author to observe that, “Collaboration increasingly seems to be the prerequisite for discovery; in other words, the scientific team has largely replaced the old ideal of the brilliant researcher working alone.”
A logical follow‐up question is whether these team efforts lead to greater impact. Wuchty attempted to address this question via an analysis of citation rates. 8 Although citation rates are not synonymous with the influence or quality of work, there is a correlation between citation rate and impact. The authors examined 19.9 million research articles on the ISI Web of Science, and 2.1 million patent records. They compared works with two or more authors to works having only one author in four major areas: science and engineering; social sciences; arts and humanities; and patents. Similar to earlier authors, 6 , 7 they observed a significant increase in the average number of authors or collaborators in all fields, except the arts and humanities. They also found that multi‐authored works are cited more often, even after removing the effects of self‐citation.
Consensus Statement II
Implications of interdisciplinary science for faculty career advancement: promotion and tenure requirements should reflect the emerging value on team science and mentoring
Private foundations and government agencies have sought to encourage multidisciplinary and interdisciplinary research by issuing requests for applications that specifically demand multi/interdisciplinary approaches. In fact, 25%–35% of current NIH and NSF RFA’s incorporate the terms “multidisciplinary” or “interdisciplinary” in the announcement. Nevertheless, there remains a significant concern that the reward systems currently in place in academia (systems for hiring, promotion, and tenure) have not kept pace with the evolution of scholarship. 1 , 9 , 10
A National Academy of Science (NAS) report on facilitating interdisciplinary research, surveyed more than 500 faculty, administrators, students, postgraduate scholars, and funding agency representatives to assess their attitudes and experiences with interdisciplinary research.1 When asked to cite the top five important impediments to interdisciplinary research at their home institutions, the most common response was promotion criteria (17%). Interestingly, 19% of provosts expressed the view that “promotion criteria” posed an impediment to interdisciplinary research (second only to “space”). The reasons most often given for this concern include the high networking costs involved in conducting interdisciplinary science, the longer start‐up required and the adverse impact on productivity, and the difficulty in distinguishing individual contributions from multiauthored team science papers.
In a separate survey of faculty and postgraduate students affiliated with six different NSF‐funded interdisciplinary research centers and programs, 30% of respondents indicated that they feared their affiliation “had not helped and in some cases had even hindered,” their career advancement. 9 Another small‐scale survey of faculty members belonging to the Council of Environmental Deans and Directors was conducted, which assessed the degree to which universities had established new policies and practices for hiring and promotion of interdisciplinary scholars. Only 16% of the responding institutions stated that they had codified procedures, with another 21% stating that new procedures were in development, but not yet in place. Nearly two‐third of institutions had not made or even considered such changes. 10
We concluded that if interdisciplinary science and the promise it holds for improving health are to be adequately promoted, then support for interdisciplinary faculty must be developed. Recognition and rewards for interdisciplinary work must be as substantial as reductionist efforts. Until then, senior faculty cannot in good conscience encourage junior faculty to embark on career paths that are perceived as less valued. This “cultural shift” is expected by all institutions funded by the national CTSA consortium. There are several types of changes that institutions might consider. Pfirman has given considerable attention to this issue, and has generated a number of thought‐provoking suggestions ( Table 2 ).
Table 2.
Recommendations to promote interdisciplinary research.
| Begin to support interdisciplinary scholars with joint appointments in two or more units from the moment they are hired, with a “letter of appointment” that explicitly addresses the appointee’s rights and duties within each reporting unit. |
| Establish promotion and tenure review committees that include members from all departments and disciplines relevant to the candidate’s career path. |
| Require that reviewers on promotion and tenure committees assign equal weight to work outside as well as within the home department. |
| Actively advise young interdisciplinary scholars on strategies for achieving a balance in the publications that support interdisciplinary research and those that demonstrate evidence of independence |
| Revise teaching policies to give greater credit to faculty who co‐teach courses across different departments. |
| Ensure that expectations for faculty members are clearly agreed upon from the start of service and share the details of this agreement with promotion and tenure review committees. |
| Invite external experts with similar interdisciplinary interests as the candidate to join promotion and tenure committees. |
| Anticipate reviewers’ concerns regarding a faculty member’s independence and productivity by modifying promotion and tenure dossiers to address frequently cited concerns. |
Several institutions have begun forward‐thinking, precedent‐setting actions that will be carefully monitored, evaluated, and reported so that other institutions might consider their costs and benefits.
Consensus Statement III
The trajectory of training physician scientists includes a long‐term commitment by institutions
The trajectory of training should involve multiple pathways to success beginning with different opportunities for medical students and postgraduate opportunities for physician scientists.
Medical students have the opportunity to engage in either a 1‐year research experience (e.g., Ruth L. Kirschstein National Research Service Award (NRSA) Institutional Research Training Grants (T32) or Clinical Translation Science Award (CTSA) T32, Howard Hughes Medical Institute, etc.) or a longer experience that culminates in a Ph.D. degree. National data on the outcomes of the physician scientist training programs, which are eagerly awaited, might refine the debate on the value of the programs. 11 Each of these opportunities includes a considerable gap between medical school training and postgraduate training. Many students may find it difficult to resume their research after clinical training. Systematic support including planned handoffs and bridge funding is necessary, especially as they may change institutions.
Similar gaps represent transitions in postgraduate training that could derail the trajectory of physician scientists. Although there are many training models, one idealized pathway is for physician scholars to begin their first research postdoctoral experience at the end of a clinical fellowship in an immersion experience anchored by membership within a 2‐year Mentored Clinical Research Training Programs (MCRTP/K30). Most will use this program to learn the rudiments of research methods and the state of the art in their field. A second mentored postdoctoral experience in the form of a K12 or similar support mechanism is often necessary. The length of the K12 varies, with some programs offering up to 5 years of support with the expectation that R‐type funding would follow. Many postdoctoral scholars will need 6–8 years of support. An idealized scheme would include 1–3 years of K12 support and 3–5 years of K23/K08 support, although the NIH offers combined K support up to 6 years with an option to appeal for two additional years.
The success of the K to R transition has been intensely discussed including one report of low conversion rates and gender disparities. 12 The gender disparities have been reevaluated. 13 Although significant differences cannot be minimized and deserve additional efforts, no difference in the success rate of K to R transition of men compared to women was observed.
This working group reviewed the results of K to R transition. The NIH data has been updated through February 2011. 14 , Figure 1 data shows that for those K08 awards awarded between 1990 and 2010, subsequent R funding, depicted by the green bars, shows steady levels of 50% or more up through 2001 (and gradually reduced later, corresponding to more recent awards). Figure 2 shows similar data for K23 awardees with successful conversion exceeding 50%. In fact, the success rate of K awardees to research project grants is very high with the median time for K23 and K08 being 4.4 and 6.0 years, respectively. The time to maximum success underscores the need for up to 8 years of support by NIH, keeping in mind that most K awardees salaries are supplemented by institutional support and additional pilot project funding.
Figure 1.
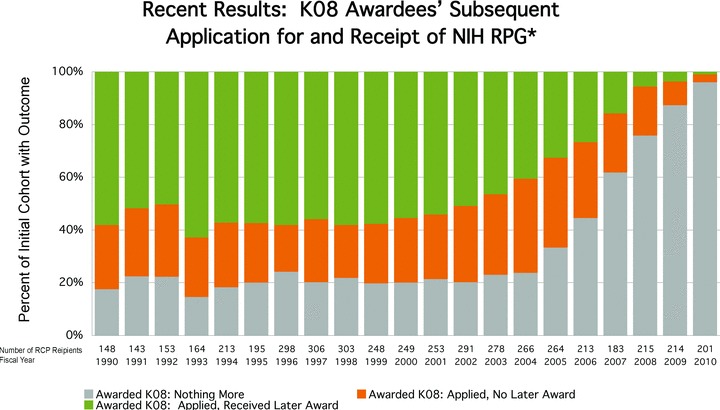
Recent result: K08 awardees’ subsequent application for and receipts of NIH Research Program Grant (RPG). RPGs include DP1, DP2, DP3, DP4, P01, P42, PN1, R01, R03, R15, R21, R22, R23, R29, R33, R34, R35, R36, R37, R55, R56, RC1, RC2, RC3, RC4, U01, U19, UC1, and UC7 mechanisms.
Figure 2.

Recent result: K23 awardees’ subsequent application for and receipts of NIH Research Program Grant (RPG). RPGs include DP1, DP2, DP3, DP4, P01, P42, PN1, R01, R03, R15, R21, R22, R23, R29, R33, R34, R35, R36, R37, R55, R56, RC1, RC2, RC3, RC4, U01, U19, UC1, and UC7 mechanisms.
Among those who could be followed for at least a decade, K awardees had a higher percentage of years with subsequent NIH support and were more likely to apply for and receive at least one competitive renewal of an R01 grant than comparable unfunded applicants. Collectively, researchers who had held a prior K01, K08, or K23 award had a significantly higher R01 award success rate than the pool of individuals with no prior career development support; K awards appeared to have the greatest impact on the subsequent NIH research involvement of M.Ds, followed by M.D./Ph.Ds and then Ph.Ds. Some unfunded applicants achieve distinction as co‐investigators or in implementation science, informatics, and medical education. 15
Consensus Statement IV
Discipline‐specific training is still required but curricula designed to promote teamwork and interdisciplinary training will promote innovation
If we agree that clinical and translational scientists need to learn to work in multidisciplinary teams, then we have to turn our attention to how well they are trained to do so. We must identify the skills required for career advancement, and the best ways to deliver those skills. A key question is that of the balance between disciplinary and interdisciplinary training. A NSF report noted, a strong interdisciplinary team depends upon both “disciplinary capability and interdisciplinary conversance.” 16 This would argue that training should develop strong disciplinary skills, along with the mindset and competencies required for success in interdisciplinary collaboration. The best interdisciplinary teamwork will not make a successful scientist if he or she is lacking disciplinary expertise to contribute to a research project; there is already the risk of interdisciplinary science being seen as “inferior” by pure disciplinarians, 17 and lack of disciplinary expertise only exacerbates that risk. Assuming that most training programs provide adequate disciplinary training, the next step is to enrich the curriculum so that trainees gain the ability to work well in interdisciplinary teams.
Many aspiring scientists pursue training through formal training programs, such as those sponsored by the CTSA and other NIH award mechanisms. These programs aim to impart skills to enable young researchers to succeed in proposing, designing, conducting, interpreting, and disseminating the results of high‐quality, relevant, ethical studies. Significant effort has already been devoted to developing the competencies for Master’s degree candidates in clinical and translational science. The major domains of competencies developed by the EdCD Key Function Committee of the CTSA are found in Table 3 and two directly address interdisciplinary competencies.
Table 3.
Major domains of competencies developed by the EdCD key function committee of the CTSA.
| Clinical and translational research questions |
| Literature critique |
| Study design |
| Research implementation |
| Sources of error |
| Statistical approaches |
| Biomedical informatics |
| Responsible conduct of research |
| Scientific communication |
| Cultural diversity |
| Translational teamwork |
| Leadership |
| Cross‐disciplinary training |
| Community engagement |
Gebbie 18 proposed a list of 17 competencies under 3 headings relating to the individual’s ability to: (i) conduct research; (ii) communicate; and (iii) interact with others. A qualitative analysis of 129 successful Integrative Graduate Education and Research Traineeship (IGERT) programs identified four domains of training for interdisciplinary collaboration: (i) grounding in multiple traditional disciplines; (ii) integration skills and broad perspective of the interdisciplinary domain; (iii) teamwork; and (iv) interdisciplinary communication. 19 These same competencies were also promoted in the NAS report on interdisciplinary research, which recommended multiple mentorships for scholars in interdisciplinary science, and training on the management of interdisciplinary projects, including “leadership and team‐working activities.” 20
How can we deliver these competencies and train young investigators to be successful in an interdisciplinary environment? Some may be fortunate enough to work with attentive mentors who will model strong disciplinary skills, interdisciplinary teamwork, and leadership. The best methods of delivery of interdisciplinary competencies, the duration of training, and the timing all remain open questions. 21 We must be mindful of the lengthy training that many clinician investigators already undergo; adding to their requirements will necessarily extend their training, and delay their ability to initiate their first study. We should seek to find ways to provide a mix of didactic and experiential learning opportunities, perhaps short‐term and periodic, that can be easily integrated into current training programs without substantially extending the duration of training. CTSA and other institutions have begun courses that are aligned with the interdisciplinary competencies and that include scholars from diverse fields of science. A comparison of their approaches and effectiveness would provide guidance to other programs.
Consensus Statement V
Ph.D. trainees can take advantage of multiple pathways to career satisfaction and success
Approximately 20% of biomedical Ph.D. graduates will pursue careers with a tenure track position and the expectation for research project grant (R) funding. 22 , 23 Many more will enjoy satisfying careers in industry, academic–industry partnerships in clinical translational research, lead administrative positions in research‐intensive universities, or teaching opportunities in colleges. Thus, the exposure to clinical and translational research during graduate and postgraduate studies is an important competitive advantage for career advancement. This position was well outlined in a recent CTSA EdCD meeting report. 24
The debate on providing graduate students more mentoring and strategic career development can be understood in the context of career options that call for individual development plans and an acknowledgment of these diverse career pathways. 25
The Ph.D. trainee should not be excluded from opportunities to: be exposed to the challenges of clinical medicine; participate in team science; pursue career development awards; and reap the benefit of expert mentoring.
Consensus Statement VI
Mentoring: centralized infrastructure and rewards will promote excellence
Academic excellence can be positively influenced by faculty mentoring programs. 26 , 27 , 28 Formal, structured mentoring programs should be fundamentally incorporated into an institution’s strategic planning process; the creation of a culture of appreciation for mentorship should be set as a goal. Key components of mentoring programs are shown in Table 4. 29 , 30 , 31 , 32
Table 4.
Essential components of mentoring programs.
| Mentor selection process for new investigators that acknowledges the need for multiple mentors and multidisciplinary teams that can change over time. 29 |
| Formal support mechanisms for research mentors that takes into account the economic, personal and time costs of mentoring. 30 |
| Training programs to improve the quality of mentoring which includes both mentee and mentor seminars. 31 |
| Ongoing assessment of the alignment of mentee and mentor expectations to foster successful mentoring. 32 |
| Formative feedback mechanisms to assist research mentors and program leaders. 33 |
Mentoring programs that utilize outcomes measures should continuously assess their effectiveness and quality. With this information, programs can modify and grow to meet the needs of both the junior faculty and their research mentors. Outcomes measured should include not only quantitative values (e.g., number of papers published, grants funded), but also qualitative job satisfaction outcomes. Strong mentor–mentee relationships can have a positive impact on specialty choice, academic career choice and retention, 32 ultimately resulting in improved job satisfaction.
Conclusions
Themes of team work and collaboration across disciplines have found their way to the popular press 33 and to very consonant themes in health sciences education. 34 The NIH has recently released a Request for Information to examine the future of the biomedical workforce. 35 Taken together the pace of discovery and improved health could advance the pace of health care and population health improvement.
Acknowledgments
This work was supported by Clinical Translational Science award and Grants: UC Davis UL1RR024146, Columbia UL1RR024156, and Northwestern UL1RR025741.
References
- 1. Committee on Facilitating Interdisciplinary Research . Facilitating interdisciplinary research. Washington , DC : National Academies Press; 2005. [Google Scholar]
- 2. Rebbeck TR, Paskett E, Sellers TA. Fostering transdisciplinary science. Cancer Epidemiol Biomarkers Prev. 2010; 19: 1149–1150. [DOI] [PubMed] [Google Scholar]
- 3. Danka‐Mullan I, Rhee KB, Stoff DM, Pohlhaus JR, Sy FS, Stinson N, Ruffin J. Moving toward paradigm shifting research in health disparities through translational, transformational, and transdisciplinary approaches. Am J Public Health. 2010; 100: S19–S24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Zerhouni E. The NIH Roadmap. Science. 2003; 302: 63–72. [DOI] [PubMed] [Google Scholar]
- 5. Meyers FJ. Recombinant innovation and translational science trainees. Sci Transl Med. 2010; 2: 39ed5. [DOI] [PubMed] [Google Scholar]
- 6. Weeks WB, Wallace AD, Surott Kimberly BC. Changes in authorship patterns in prestigious US medical journals. Soc Sci Med. 2004; 59: 1949–1954. [DOI] [PubMed] [Google Scholar]
- 7. Baethge C. Publish together or perish. Dtsh Arztebl Int. 2008; 105: 380–383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Wuchty S, Jones BF, Uzzi B. The increasing dominace of teams in production of knowledge. Science. 2007; 316: 1036–1039. [DOI] [PubMed] [Google Scholar]
- 9. Rhoten D. Interdisciplinary research: trend or transition. Items Issues. 2004; 5: 6–11. [Google Scholar]
- 10. Pfirman SL, Colins JP, Lowes S, Michaels AF. To thrive and prosper: hiring, supporting, and tenuring interdisciplinary scholars. Project Kaleidoscope Resource. 2005. Available at:http://www.pkal.org/documents/Pfirman_et‐al_To‐thrive‐and‐prosper.pdf). [Accessed April 30, 2009].
- 11. Rosenberg LE. MD/PhD programs—a call for an accounting. JAMA. 2008; 300: 1208–1209. [DOI] [PubMed] [Google Scholar]
- 12. Jagsi R, Motomura AR, Griffith KA, Rangarajan S, Ubel PA. Sex differences in attainment of independent funding by career development awardees. Ann Intern Med. 2009; 151: 804–811. [DOI] [PubMed] [Google Scholar]
- 13. Polhaus JR, Jiang H, Wagner RM, Schaffer WT, Pinn VW. Sex differences in application, success, and funding rates for NIH extramural programs. Acad Med. 2011; 86: 759–767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. NIH data review 2011. Office of Research Information systems (ORIS) division of Information Services (DIS): Reporting Branch. Available at:http://www.report.nih.gov. [Accessed February 28, 2011].
- 15. NIH Individual Mentored Career Development Awards Program evaluation report March 2 , 2011; Office of Extramural Research.
- 16. Van Hartesveldt C, Giordan J, eds. (2008). Impact of transformative interdisciplinary research and graduate education on academic institutions. Conference on Impact and Role of IGERT , May 20–21. Arlington, VA ; 2008 National Science Foundation, Education and Human Resources Directorate, Division of Graduate Education, Integrative Graduate Education and Research Traineeship (IGERT) Program. [Google Scholar]
- 17. Stein REK, Jessop, DJ . Thoughts on interdisciplinary research. J Clin Epidemiol. 1988; 41: 813–815. [DOI] [PubMed] [Google Scholar]
- 18. Gebbie KM, Meier BM, Bakken S, Carrasquillo O, Formicola A, Aboelela SW, Glied S, Larson E. Training for interdisciplinary health research: defining the required competencies. J Allied Health. 2008; 37: 65–70. [PubMed] [Google Scholar]
- 19. Borrego, M , Newswander CY. Definitions of interdisciplinary research: towards graduate‐level learning outcomes. Rev of High Educ. 2010; 34: 61–84. [Google Scholar]
- 20. National Academies (U.S.) , Committee on Facilitating Interdisciplinary Research, Committee on Science Engineering and Public Policy (U.S.), National Academy of Sciences (U.S.), National Academy of Engineering., Institute of Medicine (U.S.). Facilitating Interdisciplinary Research; Washington , DC : National Academies Press; 2005. [Google Scholar]
- 21. Hackett, EJ , Rhoten, DR . The Snowbird Charrette: integrative interdisciplinary collaboration in environmental research design. Minerva. 2009; 47: 407–440. [Google Scholar]
- 22. Available at:https://www.aamc.org/students/considering/exploring_medical/research/phd/career_paths/[Accessed May 30, 2011].
- 23. Jackson RD, Gabriel S, Pariser A, Feig P. Training the translational scientist. Sci Transl Med. 2010; 2: 63mr2. [DOI] [PubMed] [Google Scholar]
- 24. Mervis J. Reshuffling Graduate Education Science 2009; 325: 528–530. [DOI] [PubMed] [Google Scholar]
- 25. Mervis J. NIH report urges greater emphasis on training for all graduate students. Science. 2011; 331: 525. [DOI] [PubMed] [Google Scholar]
- 26. Rammanan RA, Phillips RS, Davis RB, Silen W, Reede JY. Mentoring in medicine: Keys to satisfaction. Am J Med. 2002; 112(4): 336–341. [DOI] [PubMed] [Google Scholar]
- 27. Burnham E, Fleming M. Selection of research mentors for K funded scholars. Clin Transl Sci. 2011; 4(2): 87–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Burnham E, Schiro S, Fleming M. Mentoring K scholars: strategies to support research mentors. J Clin Transl Sci. 2011; 4: 199–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Pfund C. The merits of training mentors. Science. 2006; 311: 473–474. [DOI] [PubMed] [Google Scholar]
- 30. Huskins C, Silet K, Weber‐Main AM, Begg M, Fowler V, Hamilton J, Fleming M. Identifying and aligning expectations in a mentoring relationship. Clin Transl Sci. 2011; 4: 439–447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Meagher E, Taylor L, Probstfield J, Fleming M. Evaluating research mentors working in the area of clinical translational science: a review of the literature. Clin Transl Sci. 2011; 4: 353–358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Sambunjak D, Straus SE, Marusic A. Mentoring in academic medicine: a systematic review. JAMA. 2006; 296: 1103–1115. [DOI] [PubMed] [Google Scholar]
- 33. Lehrer J. Sunset of the solo scientist. The Wall Street Journal; Feb 5, 2011. [Google Scholar]
- 34. Interprofessional Education Collaborative Expert Panel . Core competencies for interprofessional collaborative practice: Report of an expert panel. Washington, DC : Interprofessional Education Collaborative; 2011. [Google Scholar]
- 35. Request for Information (RFI): Input into the Deliberations of the Advisory Committee to the NIH Director Working Group on the Future Biomedical Research Workforce. (2011). National Institutes of Health; Available from:http://grants.nih.gov/grants/guide/notice‐files/NOT‐OD‐11‐106.html[Accessed on August 31, 2011]. [Google Scholar]