
Fig. 2.
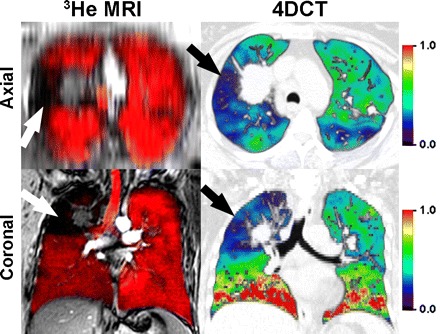
Hyperpolarized 3He-MRI coregistered with 1H-MRI as well as 4DCT acquired within 7 days in a single non-small cell lung cancer patient. Top: axial reconstructions; bottom: coronal slices. Magnetic resonance imaging (MRI) was obtained in the coronal plane during inspiration breath hold, after inhalation of a 1 liter gas mixture of hyperpolarized 3He and ultra-high purity N2 gas from functional residual capacity. 1H-MRI preceded 3He-MRI by ∼5 min and the 1H- and 3He-MRI slices were rigidly coregistered using the carina for fiducial landmarks. To generate the 4DCT ventilation maps, first, thoracic CT images were acquired during a single tidal breathing maneuver (120 kV, 60–120 mA, rotation time of 0.5 s, 360° reconstruction, pitch <0.1). CT images were reconstructed at 10 different respiratory phases and tagged as a percent of full inspiration, with in plane resolution of 1.0 mm. Deformable image registration methods were used to generate a ventilation map. Coregistered 1H (gray scale)- and 3He-MRI gas distribution images show gas in red, and focal ventilation defects are clearly shown where the 1H thoracic cavity is exposed (in black) in the absence of gas. 4DCT ventilation maps are color-coded differently such that red, orange, and yellow correspond to regions of greater ventilation; and blue, purple, and black correspond to regions of lower or no ventilation with green representing average values. Note that there is a qualitative regional correspondence between 4DCT regions of decreased ventilation and MRI regions of ventilation defects.