
Fig. 4.
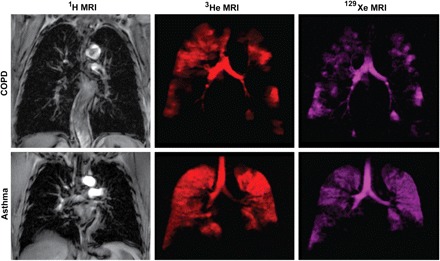
Conventional 1H-, hyperpolarized 3He- and 129Xe-MRI of a single subject each with COPD and asthma. 1H-MRI of the thoracic cavity (gray scale) was obtained in the coronal plane during inspiration breath hold, after inhalation of 1 liter of ultra-high purity N2 gas from functional residual capacity (FRC). Within 3 min, the same subject inhaled a 1 liter mixture of hyperpolarized 3He gas mixed with N2 gas from FRC for static ventilation imaging of 3He gas distribution (shown in red) acquired in a 15 s breath hold. Approximately 3 min later, the subject inhaled a 1 liter mixture of hyperpolarized 129Xe gas mixed with 4He from FRC for static ventilation imaging of 129Xe gas distribution (shown in purple) acquired in a 15 s breath hold. Note the qualitative differences in gas distribution abnormalities that are obvious between 129Xe- and 3He-MRI for both subjects. It is also important to note that the exact etiology of such gas distribution abnormalities has not yet been established. Such differences between 3He- and 129Xe-MRI gas distribution may be attributable to differences in the gas properties such as diffusion, viscosity, or perhaps tissue solubility.