
Figure 5 (A-H).
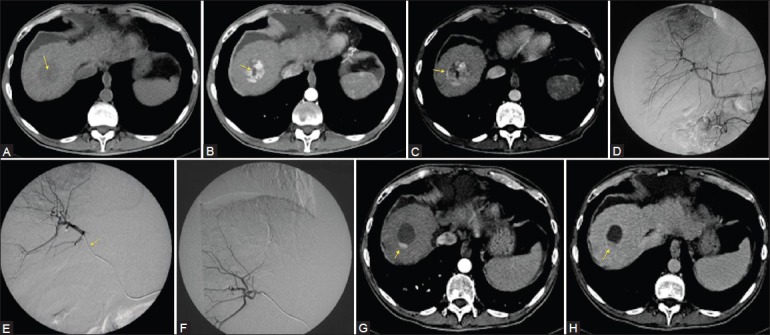
Fifty-year-old male with chronic HBV-related infection. A computed tomography (CT) exam shows the presence of a solid nodule in the VIII segment with a central necrotic area in precontrast phase (arrow) (A). After contrast injection, arterial phase (B) show enhancement of the solid part of the nodule, and confi rmed the central necrotic area (arrow). In venous phase, wash-out with a pseudocapsule formation typical of an HCC nodule (C, arrow) are noted. Angiographic exam confi rmed a correspondent hypervascular area within the VIII segment (D). After superselective catheterization, the nodule with a microcatheter (E, arrow) has been embolized with 4 ml of DC-Beads (dimensions of 100-300 μm and 300-500 μm loaded with 25 mg/ml of doxorubicin cloridrate) (F). After 1 month of follow-up, CT showed residual hypervascular area considered as pathologic finding due to the enhancement in arterial phase (G, arrow) and wash-out in late phase (H, arrow) as compared with the original CT-exam, reduction of 75% of the hypervascular area was calculated: The patient was considered in Partial Response (PR) for both EASL and mRECIST criteria