
FIGURE 5. Behavioral analyses of ‘non-spatial’ deficits in neglect patients and healthy adults.
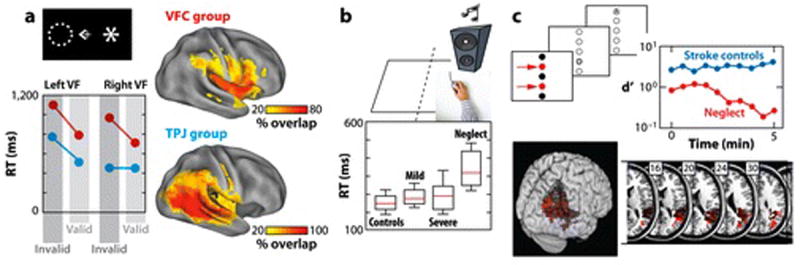
A) Reorienting deficits in neglect patients with VFC and TPJ lesions (Rengachary et al in press). Patients detected a visual target (the asterisk) that occurred in a validly cued location (indicated by the dotted circle) or at an invalidly cued location (shown in the figure). Both TPJ and VFC patients showed large contralesional deficits in reorienting, as indexed by longer RTs to unattended (invalid) than attended (valid) targets. The VFC group additionally showed reorienting deficits in the ipsilesional field and larger overall detection deficits. Similar results were observed for accuracy (not shown), but the TPJ group showed evidence of a small reorienting deficit in the ipsilesional field. B) Detection deficits in neglect patients. Neglect patients show abnormally slow simple RTs to an ipsilesional auditory stimulus (Samuelsson et al 1998). Controls were healthy age- and gender-matched subjects. The mild and severe groups consisted of non-neglect patients with minor and major right hemisphere strokes. C) Arousal deficits in neglect patients. Parietal neglect patients show a vigilance decrement (red curve) in a task that involved detection of letter targets in two locations (indicated by arrows) within a central column. No deficit is observed in right hemisphere patients without neglect (green curve). The anatomical images show the association of damaged voxels in right TPJ with the vigilance decrement, with darker areas indicating a weaker association (Malhotra et al 2009).