

Abstract
Background and Objectives:
Pit and fissure sealants are highly effective in preventing occlusal caries. The present study clinically evaluated and compared the retention and development of caries when sealed with moisture-tolerant resin-based sealant, conventional resin-based sealant with and without a bonding agent, and Glass Ionomer Cement Sealant in young permanent teeth.
Materials and Methods:
A total of 80 healthy cooperative children aged 6-9 years who were at high caries risk with all four newly erupted permanent first molars were included in the study. Teeth were divided into 4 groups using a full-factorial design, and each of the molars was sealed with the four different sealant material. Evaluation of sealant retention and development of caries was performed at 6 and 12 months using Modified Simonsen's criteria. The data obtained were tabulated and subjected to statistical analysis using Kruskal-Wallis Test and Mann-Whitney Test.
Result and Conclusion:
The result from the present study indicated that moisture-tolerant resin-based sealant could be successfully used as a pit and fissure sealant because its hydrophilic chemistry makes it less technique sensitive and simplifies the sealant application procedure.
Keywords: Bonding agent, conventional resin-based sealants, glass ionomer sealant, moisture-tolerant resin-based sealant, retention
Introduction
Pit and fissure sealants has proved to be an effective method in reducing the rate of occlusal caries on permanent posterior teeth by forming a barrier between the tooth surface and the oral environment.[1] The clinical efficacy of fissure sealants is directly related to their retention.[2] Most of the sealant materials used today are resin-based materials that possess high retention rates, but are clinically limited by the difficulties inherent in the use of resins in a moist environment because they are Bis-GMA based materials, which are primarily hydrophobic in nature and require a dry field.[3]
Delton FS+ and Clinpro Sealants are BisGMA containing visible-light cured fluoride-releasing pit and fissure sealants having superior wear resistance, better retention, and increased fluoride release. GC Fuji VII is a high fluoride-releasing, self-cure glass ionomer cement that can be light cured to hasten the final setting reaction. It has the advantage of very high fluoride release along with antibacterial property, free-flowing consistency, and improved adherence to enamel.
Although, glass ionomer and resin-based materials have been used routinely; their major drawback is retention and sensitivity to moisture, respectively. Hence, a moisture-tolerant resin sealant is necessary to ensure optimal retention.
Embrace WetBond sealant is a unique moisture-tolerant resin-based sealant that contains no BisGMA and no Bisphenol A and uses hydrophilic resin chemistry.[3] Embrace incorporates di-tri and multifunctional acrylate monomers into an advanced acid-integrating chemistry that is activated by moisture.[4] The advantages are wet-bonding, tooth-integrating, better retention, superior marginal seal, smooth margins, less technique sensitive, and increased fluoride release.[3]
This study was done to clinically evaluate and compare the retention and development of caries when sealed with moisture-tolerant resin-based, conventional resin-based sealant with a bonding agent and without a bonding agent, and Glass Ionomer Cement used as pit and fissure sealant over a period of 1 year.
Materials and Methods
The present study was carried out on 80 healthy cooperative children (37 girls, 43 boys) aged between 6 and 9 years. Caries risk assessment was conducted using American Academy of Pediatric Dentistry Caries-risk Assessment Tool 2006 (CAT) and those patients who belonged to high-risk group were included in the present study. The participating children and their parents were informed about the protocol of the study and prior parental consent was obtained.
Pit and fissure sealant application was conducted by a single operator. A thorough oral prophylaxis of both upper and lower arches was done, followed by polishing using a slurry of pumice and rotating brush to ensure removal of debris from fissures. The occlusal surfaces were then thoroughly cleaned with water to remove all traces of pumice. Isolation of permanent first molars was obtained using cotton rolls and a saliva ejector.
Teeth were divided into 4 groups using a full-factorial design, and each of the molars was sealed with four different sealants, wherein each sealant had an equal opportunity to seal all four first permanent molars on successive patients.
Group 1
Teeth were sealed with conventional resin-based sealant [Delton® FS+ Sealant (Dentsply)] with a bonding agent [Prime and Bond® NT™ (Dentsply)], following the manufacturer's instructions. The occlusal surface was dried and etched with 37% phosphoric acid gel for 30 s, followed by thorough rinsing for 30 s using an oil-free air-water syringe. Bonding agent (Prime and Bond® NT™) was applied on the pit and fissures, followed by air thinning and light curing for 10 s. Delton® FS+ was then applied with the brush applicator and light cured for 20 s using visible light cure unit.
Group 2
Teeth were sealed with conventional resin-based sealant without a bonding agent [Clinpro™ Sealant (3M ESPE)]. The procedure was similar to group 1 teeth with an exception of not applying a bonding agent.
Group 3
Teeth were sealed with moisture-tolerant resin-based sealant [Embrace™ Wetbond™ Sealant (Pulpdent Corporation)] following the manufacturer's instructions. The occlusal surface was acid etched with 37% phosphoric acid for 15 seconds. The teeth were then rinsed with copious water to remove all etching gel with air water spray. After rinsing, the teeth were lightly dried with a cotton pellet to remove excess water but were not desiccated. The occlusal surface of the teeth remained slightly moist and appeared glossy and shiny prior to the application of the sealant material. Embrace pit and fissure sealant was applied to the pits and fissures with a small applicator tip attached to the syringe. The sealant was then light-cured for 20 s using visible light cure unit.
Group 4
Teeth were sealed with Glass Ionomer Cement [GC Fuji VII Glass Ionomer Cement (GC Corporation)] following the manufacturer's instructions. The occlusal surfaces were conditioned with GC Dentin Conditioner for 20 s and then rinsed for another 20 s, followed by drying by blotting with a cotton pellet and gently blowing with an air syringe. The surfaces appeared moist and not desiccated. Fuji VII cement was then applied to the occlusal surface using a plastic-filling instrument and a disposable nylon brush to spread it into the pits and fissures. The sealant was protected with a coat of petroleum jelly after the initial set of glass ionomer sealant.
Articulating paper was used to check the occlusion and any premature contacts were adjusted. The patients were instructed not to eat or drink anything for 30 min, and not to bite or chew on hard substances for the rest of the day. The patients were recalled after a time interval of 6 and 12 months to evaluate the retention and development of caries using Modified Simonsen's criteria.[5]
Criteria for evaluation: (Modified simonsen's criteria)
Score 0: No loss of sealant and no evidence of caries
Score 1: Partial loss of sealant and no evidence of caries
Score 2: Partial loss of sealant and evidence of caries
Score 3: Complete loss of sealant and no evidence of caries
Score 4: Complete loss of sealant and evidence of caries.[5]
On recall at 6th and 12th month interval, the sealants were evaluated by visual and tactile examination with a sharp probe for retention. The teeth were visually inspected for caries. The data obtained were tabulated and subjected to statistical analysis using Kruskal-Wallis test and Mann-Whitney test.
Results
Of the 80 children whose teeth were sealed (320 sealed upper and lower first permanent molars), 4 children (16 sealed upper and lower first permanent molars) dropped out of the study after 6 month interval as they left the city; 76 children (304 sealed upper and lower first permanent molars) were evaluated at 12-month interval.
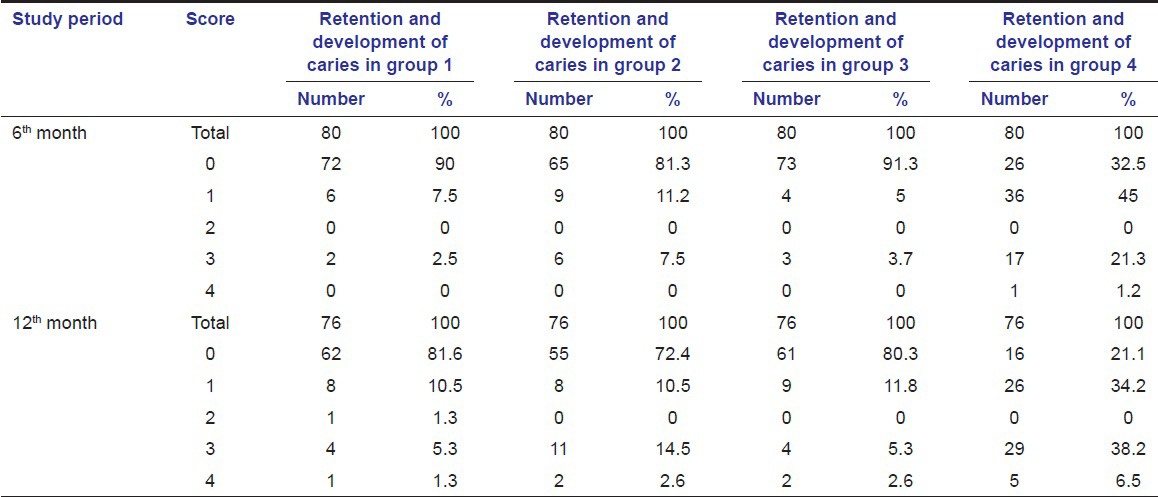
Table 1 shows the distribution of scores for retention and development of caries among the four groups.
Table 1.
Retention and development of caries in Groups 1-4
At 6-month follow-up, the lowest mean score was seen in conventional resin-based sealant with a bonding agent (0.15) and moisture-tolerant resin-based sealant (0.16), followed by conventional resin-based sealant without a bonding agent (0.34); the highest mean score was seen in Glass Ionomer Sealant (1.14). At 12-month follow-up, the lowest mean score was again seen in conventional resin-based sealant with a bonding agent (0.34), followed by moisture-tolerant resin-based sealant (0.38), conventional resin-based sealant without a bonding agent (0.64), and Glass Ionomer Sealant (1.75). The difference in the mean scores between the four groups was found to be statistically significant (P < 0.001) at both 6th and 12th month interval [Table 2].
Table 2.
Comparison of resin-based and glass ionomer sealants for the retention and development of caries at 6 and 12 months

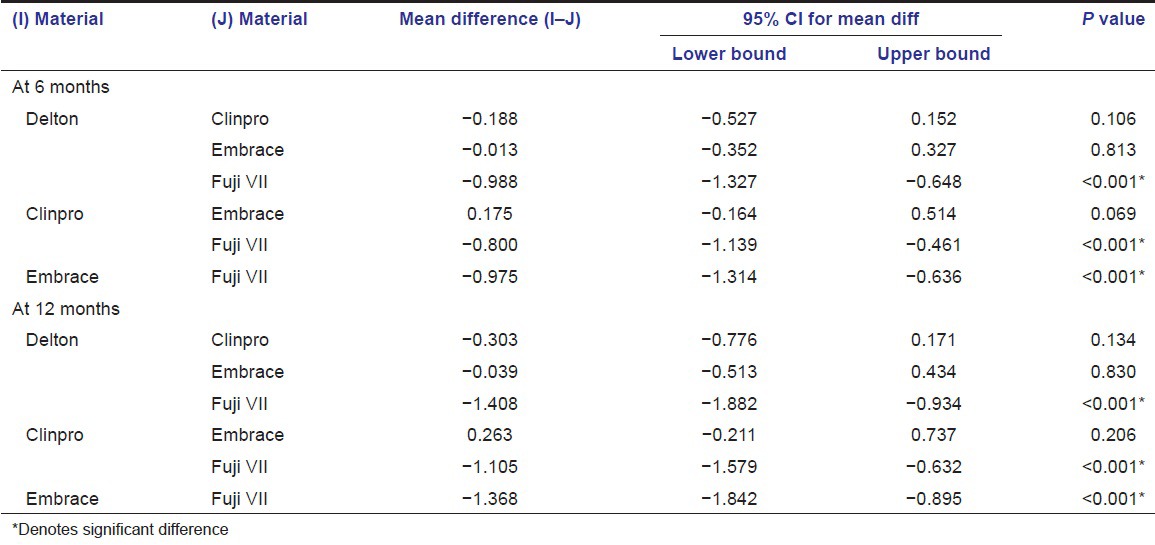
At both 6th and 12th month follow-up, the difference in the mean score was found to be statistically significant between Glass Ionomer Sealant and conventional resin-based sealant with a bonding agent, conventional resin-based sealant without a bonding agent, and moisture-tolerant resin-based sealant (P < 0.001). However, there was no statistically significant difference in the mean score between conventional resin-based sealant with a bonding agent, conventional resin-based sealant without a bonding agent, and moisture-tolerant resin-based sealant [Table 3].
Table 3.
Multiple comparisons of resin-based and Glass Ionomer Sealants for the retention and development of caries at 6 and 12 months using Mann-Whitney test
Discussion
Pit and fissure sealants are an important part of caries-preventive strategies.[6] The rationale for the use of sealants as a preventive intervention is the high prevalence of pit and fissure caries. When applied to deep, caries-prone fissures, pit and fissure sealants penetrate and protect the vulnerable areas from the oral environment.[7] Clinical studies have shown that, with the application of fissure sealants, an additional reduction in caries development was achieved as compared to untreated controls.[8,9]
Since the inception of fissure sealant, a number of sealants have been developed and tested for their effectiveness. These sealants differ in the base material used, the method of polymerization, and whether or not they contain fluoride. Currently, there are 2 basic types of sealants: Resin and glass ionomer sealants. Most of the sealant materials used today are resin-based materials that possess high retention rates. Placement of resin-based sealant is very technique sensitive and is influenced by several factors such as patient cooperation, operator variability, and contamination of the operating field.[10] However, the major drawback of fissure sealing with resins is its extreme sensitive nature to moisture, as they are Bis-GMA-based materials that are primarily hydrophobic in nature. Glass ionomers are less sensitive to moisture than resins, a fact that makes it reasonable to believe that they may be preferable for sealing newly erupted teeth.[6] Ionomeric cements are used for sealing pits and fissures, mainly due to their fluoride release and adherence to the dental structures.[11] Despite their promising results, the main disadvantage of glass ionomer sealants is its inadequate retention.[12,13] Hence, a moisture-tolerant resin sealant is necessary to ensure optimal retention.
This study evaluated and compared the moisture-tolerant resin-based sealant that contains no BisGMA (Embrace™ Wetbond™ Sealant) with conventional resin-based sealant that contains BisGMA with a bonding agent (Delton® FS+ Sealant with Prime and Bond® NT™) and without a bonding agent (Clinpro™ Sealant) and Glass Ionomer sealants (GC Fuji VII) for retention and development of caries at periodic intervals.
In the present study, the 6th month clinical evaluation showed complete retention in 90% of the conventional resin-based sealant with a bonding agent, 81.3% of conventional resin-based sealant without a bonding agent, 91.3% of moisture-tolerant resin-based sealant, and 32.5% of glass ionomer sealant. At 12 months evaluation, complete retention was seen in 81.6% of conventional resin-based sealant with a bonding agent, 72.4% of conventional resin-based sealant without a bonding agent, 80.3% of moisture-tolerant resin-based sealant, and 21.1% of glass ionomer sealant. Development of caries was seen in 2 teeth (2.6%) of groups 1-3 and 5 teeth (6.5%) in group 4 at the 12-month follow-up.
The present study showed a statistically significant difference in the mean score between Glass Ionomer Sealant (group 4) and conventional resin-based sealant with a bonding agent (group 1), conventional resin-based sealant without a bonding agent (group 2), and moisture-tolerant resin-based sealant (group 3), which is in agreement with previous studies. Songpaisan and coworkers in a field trial found retention of resin sealant to be 92% after 6 months, while retention of glass ionomer sealant was as low as 2-8%.[14] Poulsen et al., found the glass ionomer sealant to be lost in almost 90% of the teeth as compared to only 10% of resin sealant after 3 years.[15] One main reason for the loss of the glass ionomer sealants could be inadequate adhesion of the cement to the enamel surface.[12] Glass ionomers formulated as lining materials may have inferior solubility resistance and abrasion resistance in the mouth.[16] The low wear resistance of glass ionomer materials to occlusal forces may contribute to a faster cement disintegration, thinning the sealant, and eventually fracturing it off the enamel surface.
The present study showed that there was marginally higher retention of resin-based sealants when bonding agents were used prior to sealant application; however, the difference was not statistically significant. Similar results have been reported from other studies. Boksman et al.,[17] compared the retention rate of a filled and an unfilled sealant with and without the use of two bonding agents under in vivo settings. After 2 years, they concluded that using bonding agents did not increase the retention of either types of sealant. Locker after an evidence-based study recommended that placing a bonding agent prior to the sealant on the surface does not appear to enhance retention rates.[18] However, studies have also shown that dentin bonding agents increased the retention of sealants, especially in cases where saliva/water contamination was unavoidable.[2,19,20] It can be speculated that the benefit of this primer and adhesive layer under the sealant is based on a combination of moisture-chasing effects of the hydrophilic primers, increased flow imparted by the less viscous primer and adhesive and increased flexibility of the combined and polymerized primer/adhesive/resin complex once complete.[21] Although not contraindicated, considering the extra time and cost needed and the inconclusive reports in retention, routine use of a bonding agent as part of the sealant application technique is not recommended.[18]
Success of a pit and fissure sealant mainly depends on its caries-preventive effect.[6] The current study measured the effectiveness of the sealant by its ability to prevent caries in the sealed surfaces of permanent first molars in children considered to be at a high risk for dental caries. No significant difference was seen in the development of caries between the 4 groups at 12th month evaluation, though it was marginally higher in glass ionomer sealant group. Further evaluation over an extended time period is required to assess the occurrence of caries, especially on those teeth in which sealants have been partially or completely lost.
Embrace WetBond sealant is a unique moisture-tolerant resin-based sealant that is activated by moisture.[4] When activated, the material is acidic, and, in cured state, it is no longer affected by water and, as a result, cured material has a neutral pH and very low water solubility.[22] In vitro studies[22,23] on Embrace wet bond have shown that the material is less viscous, forms longer resin tags, and shows less microleakage, superior marginal adaptation, and excellent penetration into fissures as compared to conventional Bis-GMA-based sealants. Longitudinal study by O’Donnell[24] revealed that 95% of the sealants remained intact with a good marginal integrity and 100% were caries-free at the end of 2 years.
The result from the present study showed no significant difference between moisture-tolerant resin-based sealants and conventional resin-based sealants in both retention and development of caries. Thus, it indicates that moisture-tolerant resin-based sealant could be a boon to pit and fissure sealants in Pediatric Dentistry. Since moisture contamination is a significant risk factor to sealant retention, the introduction of a moisture-tolerant resin-based sealant, which is clinically successful, provides clinicians an additional choice in their preventive regimen.[24] The use of moisture-tolerant resin-based sealant could be encouraged in situations difficult to attain moisture control as it incorporates a hydrophilic chemistry. Application of moisture-tolerant resin-based sealant is highly beneficial in treating children because it is often difficult to maintain a dry field, and the fact that the material works well in a slightly moist field is a great benefit to the practitioner. The ability to bond in the presence of moisture simplifies the sealant procedure and makes it less technique sensitive. Recently, concerns have been raised about the possibility of estrogenic chemicals, especially bisphenol-A (BPA) and bisphenol-A dimethacrylate (BPA-DMA), leaching out of resin-based sealants.[25] Thus, moisture-tolerant resin-based sealant that contains no BisGMA and no Bisphenol A can be considered as a viable alternative.
Conclusion
The following conclusions were drawn from the present study:
The retention of the resin-based sealants was superior to that of the Glass Ionomer sealant that was statistically significant
The use of a bonding agent as an intermediary layer between enamel and sealant in a dry and isolated situation has no statistically significant effect on fissure-sealant retention
Moisture-tolerant resin-based sealant was as effective as conventional Bis-GMA-based sealants in terms of retention and caries prevention
Caries preventive effect of Glass Ionomer Sealant (93.5%) was almost similar to that of resin-based sealants (97.4%).
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Salama FS, Al-Hammad NS. Marginal seal of sealant and compomer materials with and without enameloplasty. Int J Pediatr Dent. 2002;12:39–46. [PubMed] [Google Scholar]
- 2.Waggoner WF, Siegal M. Pit and fissures sealant application: Updating the technique. J Am Dent Assoc. 1996;127:351–61. doi: 10.14219/jada.archive.1996.0205. [DOI] [PubMed] [Google Scholar]
- 3.Hoffman I. A moisture tolerant, resin based pit and fissure sealant. Dental Tribune Dec. 2009:17A–18A. Industry Clinical. [Google Scholar]
- 4.Strassler HE, O’Donnell JP. A unique moisture-tolerant, resin based pit-and-fissure sealant: Clinical technique and research results. Inside Dent. 2008;4:2–3. [Google Scholar]
- 5.Ganesh M, Tandon S. Clinical evaluation of Fuji VII sealant material. J Clin Pediatr Dent. 2006;31:52–7. doi: 10.17796/jcpd.31.1.w8532743883hw64n. [DOI] [PubMed] [Google Scholar]
- 6.Beauchamp J, Caufield PW, Crall JJ, Donly K, Feigal R, Gooch B. Evidence-based clinical recommendations for the use of pit-and-fissure sealants. J Am Dent Assoc. 2008;139:257–67. doi: 10.14219/jada.archive.2008.0155. [DOI] [PubMed] [Google Scholar]
- 7.Vineet D, Tandon S. Comparative evaluation of marginal integrity of two new fissure sealants using invasive and non-invasive techniques: SEM study. J Clin Pediatr Dent. 2000;24:291–7. doi: 10.17796/jcpd.24.4.74hx7311l705213j. [DOI] [PubMed] [Google Scholar]
- 8.Selwitz RH, Raymer NR, Driscoll WS, Li SH. Evaluation after 4 years of the combined use of fluoride and dental sealants. Community Dent Oral Epidemiol. 1995;23:30–5. doi: 10.1111/j.1600-0528.1995.tb00194.x. [DOI] [PubMed] [Google Scholar]
- 9.Sterritt GB, Frew RA, Rozier RG, Brunelle JA. Evaluation of a school-based fluoride mouth rinsing and clinic-based sealant program on a non-fluoridated island. Community Dent Oral Epidemiol. 1990;18:288–93. doi: 10.1111/j.1600-0528.1990.tb00082.x. [DOI] [PubMed] [Google Scholar]
- 10.Karlzén-Reuterving G, van Dijken JW. A three-year follow-up of glass ionomer cement and resin fissure sealants. ASDC J Dent Child. 1995;62:108–10. [PubMed] [Google Scholar]
- 11.Williams B, Laxton L, Holt RD, Winter GB. Fissure sealants: A 4-year clinical trial comparing an experimental glass polyalkenoate cement with a bis glycidyl methacrylate resin used as fissure sealants. Br Dent J. 1996;180:104–8. doi: 10.1038/sj.bdj.4808989. [DOI] [PubMed] [Google Scholar]
- 12.Mejare I, Mjor IA. Glass ionomer and resin-based fissure sealants: A clinical study. Scand J Dent Res. 1990;98:345–50. doi: 10.1111/j.1600-0722.1990.tb00983.x. [DOI] [PubMed] [Google Scholar]
- 13.Boksman L, Gratton DR, McCutcheon E, Plotzka OB. Clinical evaluation of a glass ionomer cement as a fissure sealant. Quintessence Int. 1987;18:707–9. [PubMed] [Google Scholar]
- 14.Songpaisan Y, Bratthall D, Phantumvanit P, Somridhivej Y. Effects of glass ionomer cement, resin-based pit and fissure sealant and HF applications on occlusal caries in a developing country field trial. Community Dent Oral Epidemiol. 1995;23:25–9. doi: 10.1111/j.1600-0528.1995.tb00193.x. [DOI] [PubMed] [Google Scholar]
- 15.Poulsen S, Beiruti N, Sadat N. A comparison of retention and the effect on caries of fissure sealing with a glass-ionomer and a resin-based sealant. Community Dent Oral Epidemiol. 2001;29:298–301. doi: 10.1034/j.1600-0528.2001.290409.x. [DOI] [PubMed] [Google Scholar]
- 16.Raadal M, Utkilen AB, Nilsen OL. Fissure sealing with a light-cured resin reinforced glass-ionomer cement (Vitrebond) compared with a resin sealant. Int J Pediatr Dent. 1995;6:235–9. doi: 10.1111/j.1365-263x.1996.tb00251.x. [DOI] [PubMed] [Google Scholar]
- 17.Boksman L, McConnell RJ, Carson B, McCutcheon-Jones EF. A 2-year clinical evaluation of two pit and fissure sealants placed with and without the use of a bonding agent. Quintessence Int. 1993;24:131–3. [PubMed] [Google Scholar]
- 18.Locker D, Jokovic A, Kay EJ. Prevention. Part 8: The use of pit and fissure sealants in preventing caries in the permanent dentition of children. Br Dent J. 2003;195:375–8. doi: 10.1038/sj.bdj.4810556. [DOI] [PubMed] [Google Scholar]
- 19.Feigal RJ, Musherure P, Gillespie B, Levy-Polack M, Quelhas I, Hebling J. Improved sealant retention with bonding agents: A clinical study of two-bottle and single-bottle systems. J Dent Res. 2000;79:1850–6. doi: 10.1177/00220345000790110601. [DOI] [PubMed] [Google Scholar]
- 20.Grande RH, de Lima AC, Rodrigues Filho LE, Witzel MF. Clinical evaluation of an adhesive used as a fissure sealant. Am J Dent. 2000;13:167–70. [PubMed] [Google Scholar]
- 21.Fiegal RJ. The use of pit and fissure sealants. Pediatr Dent. 2002;24:415–22. [PubMed] [Google Scholar]
- 22.Kane B, Karren J, Garcia-Godoy C, Garcia-Godoy F. Sealant adaptation and penetration into occlusal fissures. Am J Dent. 2009;22:89–91. [PubMed] [Google Scholar]
- 23.Prabhakar AR, Murthy SA, Sugandhan S. Comparative evaluation of the length of resin tags, viscosity and microleakage of pit and fissure sealants-an in vitro scanning electron microscope study. Contemp Clin Dent. 2011;2:324–30. doi: 10.4103/0976-237X.91797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.O’Donnell JP. A moisture-tolerant, resin based pit-and-fissure sealant: Research results. Inside Dent. 2008;4:50–52. [Google Scholar]
- 25.Tarumil H, Imazatol S, Narimatsul M, Matsuo M, Ebisu S. Estrogenicity of fissure sealants and adhesive resins determined by reporter gene assay. J Dent Res. 2000;79:1838–43. doi: 10.1177/00220345000790110401. [DOI] [PubMed] [Google Scholar]