
Fig. 2.
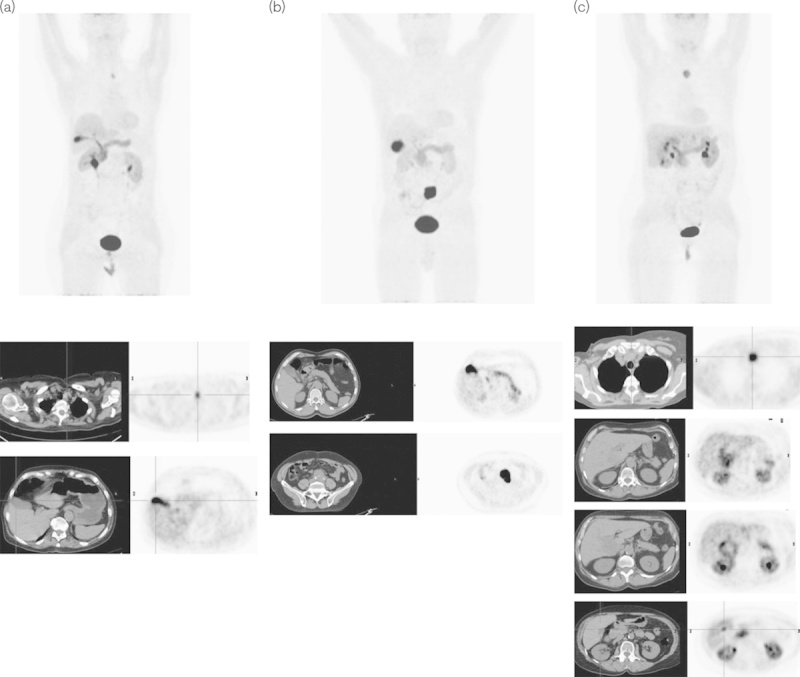
Normal variants of the l-6-[18F]fluoro-3,4-dihydroxyphenylalanine (18F-DOPA) excretion through the biliary tract. Upper series: MIP images of three patients (a–c) with medullary thyroid carcinoma (MTC) (a, c) and paraganglioma (b). Lower series: axial images of the low-dose computed tomography (CT) (on the left) and PET (on the right) of the pathologic uptake of 18F-DOPA. (a) a 78-year-old woman with MTC previously operated upon and with suspicion of relapse in the left paratracheal region well visualized at 18F-DOPA PET/CT; (b) a 68-year-old man with a suspicion of paraganglioma on morphological imaging in the aortic carefour region of the abdomen confirmed on 18F-DOPA PET/CT, which depicted an area of very high radiotracer uptake with an SUVmax of 29.9; (c) a 66-year-old woman with MTC previously operated upon, with increased calcitonin levels and hepatic and nodal metastases. In all of the above images, the variability of 18F-DOPA uptake in the physiological sites and pathologic areas, which are clearly recognized, is noteworthy. Note the very intense uptake in the gallbladder in (a) and (b), and the uptake in the biliary tracts especially in (a) and (c). In (c) note the lesions in the liver as well as the physiologic focal uptake in the gallbladder that could be misinterpreted as another hepatic lesion.