
Figure 2.
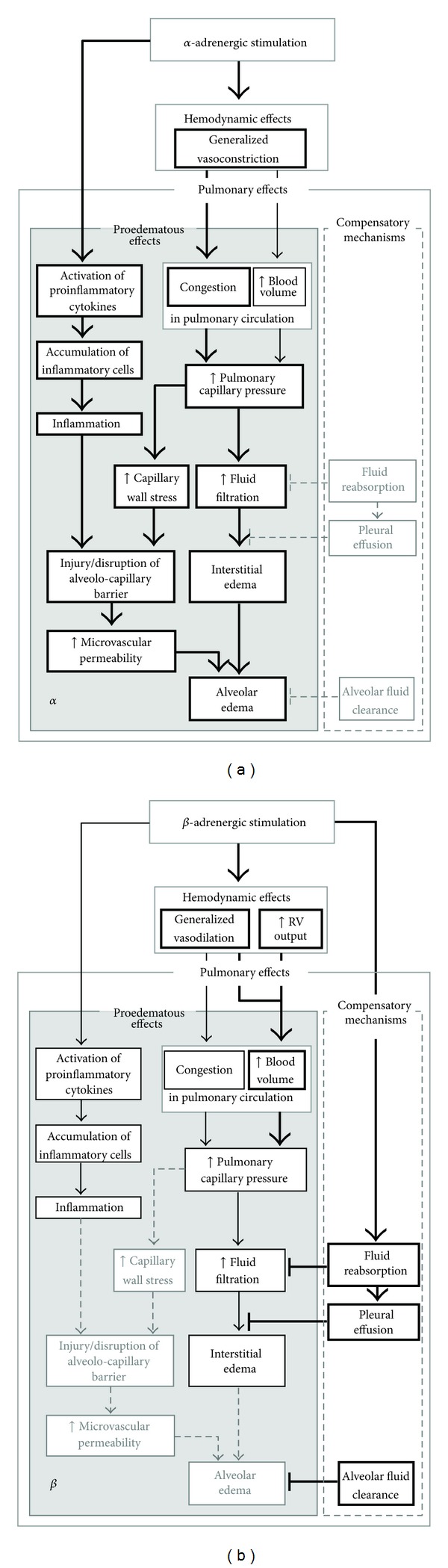
(a): Contribution of α-adrenergic stimulation to the development of pulmonary edema. Treatment with α-adrenergic agonists promotes all proedematous effects of adrenoceptor stimulation, particularly pulmonary microvascular congestion. Elevated capillary pressure and capillary wall stress increase fluid filtration. Microvascular permeability can increase due to capillary wall stress and inflammation. This may result in alveolar edema. Protective mechanisms are not advanced by α-adrenergic mechanisms. (b): Contribution of β-adrenergic stimulation to the development of pulmonary edema. Vasodilation mediated by β-adrenergic stimulation may cause blood overfilling in the pulmonary circulation and, consequently, increase pulmonary capillary pressure. This is usually less pronounced than with α-adrenergic stimulation and is not associated with increased capillary wall stress. Although β-adrenergic agonists exert anti-inflammatory effects, prolonged stimulation may induce focal inflammation. In general, with β-adrenergic stimulation edema develops slowly allowing protective mechanisms such as filtration into the pleural space to be more effective. Moreover, compensatory mechanisms such as alveolar fluid clearance are enhanced, thus preventing flooding of the alveoli. Bold arrows and boxes depict the main effects of the respective treatment; thin arrows and boxes characterize slight or less pronounced effects; dashed arrows and boxes with light-grey frames and types mark processes that are not affected or inhibited by this type of stimulation. RV: right ventricular, ↑: increase.