
4.
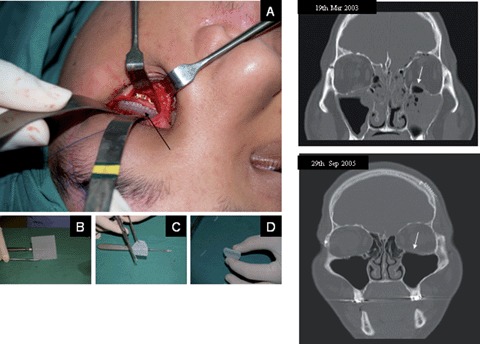
The intended clinical use defines the desired properties of engineered bone substitutes. Defects of load-bearing long bones, for instance, require constructs with high mechanical stability whereas initial plasticity is not essential. On the other hand for craniofacial applications, e.g. orbital floor fractures, moldable scaffolds (A–D) are favorable. Depending on the implantation site, initial vascularization is essential for enhanced engraftment and prevention of infections. Mechanical stability, osteoconductivity by attracting and stimulating bone-forming cells of the host bone, and ease of handling have been well balanced in the design of mPCL scaffold sheets in order to properly meet the clinician's needs. The clinical follow up 2.5 years postsurgery (lower CT image) of a patient receiving a mPCL scaffold (defect site shown in upper CT image) for the reconstruction of a orbital floor fracture defect showed complete bone regeneration of the defect site (arrow).