
Figure 1.
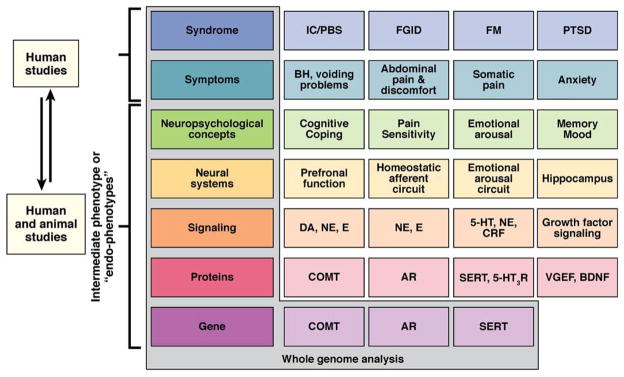
Intermediate phenotype strategy for FGIDs and frequently comorbid disorders. Shown is the progressive deconstruction of clinical, symptom-based syndromes (several examples are shown in the first row) into intermediate phenotypes (examples are shown in each row) all the way down to the genome. For clarity, only a small number of candidate genes are shown. Although the syndrome and the symptoms can only be studied in humans, the neurobiological endophenotypes can be studied both in humans and in animal models. It has been postulated that the correlation between neurobiological endophenotypes and genes is significantly higher than the correlation between clinical syndromes and genes. IC/PBS, interstitial cystitis/painful bladder syndrome; FM, fibromyalgia; PTSD, posttraumatic stress syndrome; DA, dopamine; NE, norepinephrine; E, epinephrine; CRF, corticotropin-releasing factor; COMT, catechol-O-methyltransferase; AR, adrenoreceptor; VGEF, vascular endothelial growth factor; BDNF, brain-derived neurotrophic factor. Mayer EA, Bushnell MC. Functional pain disorders: time for a paradigm shift? In: Mayer EA, Bushnell MC, eds. Functional pain syndromes: presentation and pathophysiology. Seattle, WA: IASP Press, 2009:531–565. This figure has been reproduced with permission of the International Association for the Study of Pain® (IASP®). The figure may not be reproduced for any other purpose without permission.