

Abstract
Background
Although various radiographic measurements have been developed and used for evaluating hallux valgus, not all are universally believed to be necessary and their relationships have not been clearly established. Determining which are related could provide some insight into which might be useful and which would not.
Questions/Purposes
We investigated the reliability of eight radiographic measurements used to evaluate hallux valgus, and determined which were correlated and which predicted the hallux valgus angle.
Methods
We determined eight radiographic indices for 732 patients (mean age, 51 years; SD, 17 years; 107 males and 625 females) with hallux valgus: hallux valgus angle, intermetatarsal angle, hallux interphalangeal angle, distal metatarsal articular angle, proximal phalangeal articular angle, simplified metatarsus adductus angle, first metatarsal protrusion distance, and sesamoid rotation angle. Intraobserver and interobserver reliabilities of each radiographic measurement were analyzed on 36 feet from 36 randomly selected patients. Correlations among the radiographic measurements were analyzed. Radiographic measurements predicting hallux valgus angle were evaluated using multiple regression analysis.
Results
Hallux valgus angle had the highest reliability, whereas the distal metatarsal articular angle and simplified metatarsus adductus angle had the lowest. Distal metatarsal articular angle, intermetatarsal angle, and sesamoid rotation angle had the highest correlations with hallux valgus angle. Distal metatarsal articular angle correlated with sesamoid rotation angle. The intermetatarsal angle, interphalangeal angle, distal metatarsal articular angle, first metatarsal protrusion distance, sesamoid rotation angle, and metatarsus adductus angle predicted the hallux valgus angle.
Conclusions
We suggest using hallux valgus angle, intermetatarsal angle, interphalangeal angle, sesamoid rotation angle, and first metatarsal protrusion distance considering their reliability and prediction of the deformity.
Level of Evidence
Level II, diagnostic study. See Guidelines for Authors for a complete description of levels of evidence.
Introduction
Hallux valgus is a common deformity in which the big toe primarily is deviated laterally at the metatarsophalangeal joint. However, this deformity is too complex to be evaluated at one joint on one plane. Hallux valgus occurs frequently with a medial deviation of the first metatarsal bone, a deformity on the phalangeal bone and interphalangeal joint, and pronation of the big toe with sesamoid subluxation [4].
Symptomatic hallux valgus resistant to nonoperative management is treated surgically. A range of surgical methods [4, 6, 14] has been developed to correct each component of the hallux valgus and concurrent abnormalities. In determining the appropriate surgical treatment and assessing the postoperative outcome, some authors consider radiographic evaluation an important tool [4, 6, 14]. However, most radiographic measurements focus on the angular deformities in the transverse plane, which are measured on dorsoplantar foot radiographs [4], and rotational deformities in the coronal plane have attracted relatively less attention, although the deformity is three-dimensional and the radiographic measurements in the transverse plane would likely be affected by the deformities of the coronal plane.
Numerous studies have reported the reliability of various radiographic measurements evaluating a hallux valgus deformity [3, 5, 15, 20, 21, 24]. These studies generally report reliability ranging from 0.38 to 0.99 in intraclass correlation coefficient (ICC) values. However, all these radiographic indices might not be necessary to critically assess the deformity, and the correlations between radiographic indices might help discriminate between the real and apparent deformities caused by the different projections of the radiographic images.
We therefore investigated various measures to establish (1) their reliability; (2) the relationships among the radiographic measurements on different planes; and (3) their ability to predict the hallux valgus angle.
Patients and Methods
We retrospectively reviewed 762 patients who visited our orthopaedic clinic for hallux valgus between January 2004 and May 2011 and underwent a radiographic examination. The radiographic evaluation included a weightbearing dorsoplantar foot radiograph, weightbearing lateral foot radiograph, and weightbearing sesamoid axial view radiograph. We excluded 30 patients with previous surgery of the foot and lower extremity, foot fractures, congenital malformation, neuromuscular diseases, tumors, or infections that could cause foot deformities. These exclusions left 732 patients; we used one foot from each patient (see subsequently). The mean age of the patients was 51 years (SD, 17 years), and there were 107 male and 625 female patients. The mean hallux valgus angle was 23° (SD, 11°) (Table 1). This retrospective study was approved by the Institutional Review Board at our hospital.
Table 1.
Patients’ demographics and summary of radiographic measurements
| Patients’ and radiographic information | Mean |
|---|---|
| Number | 732 |
| Age (years) | 51 (SD, 17) |
| Male:female | 107:625 |
| Right:left | 367:365 |
| Radiographic measurements | |
| HVA (°) | 23 (SD, 11; range, 5 to 70) |
| IMA (°) | 12 (SD, 4; range, 2 to 36) |
| IPA (°) | 11 (SD, 7; range, −16 to 65) |
| DMAA (°) | 11 (SD, 8; range, −10 to 62) |
| PPAA (°) | 4 (SD, 5; range, −12 to 29) |
| Metatarsus adductus (°) | 25 (SD, 6; range, 6 to 53) |
| First MT protrusion (mm) | 2 (SD, 3; range, −17 to 18) |
| SRA (°) | 9 (SD, 13; range, −22 to 60) |
HVA = hallux valgus angle; IMA = intermetatarsal angle; IPA = interphalangeal angle; DMAA = distal metatarsal articular angle; PPAA = proximal phalangeal articular angle; Metatarsus adductus = simplified metatarsus adductus angle; First MT protrusion = first metatarsal protrusion distance; SRA = sesamoid rotation angle.
We calculated the prior sample size to determine the minimum number of patients required based on reliability testing. In this study, the ICCs were used for reliability testing at a target value of 0.8 and a 95% CI of 0.2. We calculated the sample size to be 36 patients with a Bonett’s approximation [2]. One foot from each patient was selected by random sampling for statistical independence and included for data analysis [18].
The foot radiographs were taken using a UT 2000 X-ray machine (Philips Research, Eindhoven, The Netherlands) at a source-to-image distance of 100 cm and were set to 50 kVp and 5 mAs with the patients standing. We retrieved the radiographic images using a picture archiving and communication system (PACS) (IMPAX; Agfa Healthcare, Mortsel, Belgium), and radiographic measurements were performed using PACS software. The radiographic imaging and measuring system was digital.
We identified and assessed the following 14 radiographic measurements evaluating hallux valgus from a literature review: hallux valgus angle [10], intermetatarsal angle [10], distal metatarsal articular angle [19], proximal phalangeal articular angle [1], interphalangeal angle [1], first metatarsal protrusion distance [9], metatarsus adductus angle [11], simplified metatarsus adductus angle [7], first metatarsal cuneiform angle [8], tibial sesamoid position [14], tibia sesamoid-second metatarsal distance [12], sesamoid rotation angle [13], axial tibial sesamoid-second metatarsal distance [12], and axial tibial sesamoid grade [25].
These measures were selected based on the consensus of four orthopaedic surgeons (PMS, KML, KHS, TWK) with orthopaedic experience of 12, 10, 8, and 5 years, respectively. During the consensus discussion, we excluded qualitative indices such as tibial sesamoid position and axial tibial sesamoid grade. Tibial sesamoid-second metatarsal distance and axial tibial sesamoid-second metatarsal distance were believed to be affected by differences in body size and also were excluded. We also excluded other redundant measurements (first metatarsal cuneiform angle and metatarsus adductus angle). Eight of the 14 items were finally elected for the radiographic measurements. The following items were measured on the dorsoplantar foot radiographs: hallux valgus angle [10], intermetatarsal angle [10], hallux interphalangeal angle [23], distal metatarsal articular angle [19], proximal phalangeal articular angle [1], simplified metatarsus adductus angle [7], and first metatarsal protrusion distance [9]. We measured one item on the sesamoid axial view radiographs, sesamoid rotation angle [13].
Another consensus-building session was held among the three orthopaedic surgeons (KML, KHS, TWK) for reliability testing, where they agreed on the details of the methods for the radiographic measurements.
On the dorsoplantar foot weightbearing radiographs, the hallux valgus angle is the angle between the longitudinal axis of the first metatarsal and that of the proximal phalanx [10]. The intermetatarsal angle was the angle between the longitudinal axis of the first and second metatarsals [10]. The hallux interphalangeal angle was the angle between the longitudinal axis of the proximal phalanx and the distal phalanx of the hallux [23]. The proximal phalangeal articular angle was the angle between a line perpendicular to the longitudinal axis of the proximal phalanx and a line delineating the orientation of the proximal phalangeal base articular surface [1]. The simplified metatarsus adductus angle was defined as the angle between the longitudinal axis of the second metatarsal and the longitudinal axis of the middle cuneiform [7] (Fig. 1). The distal metatarsal articular angle was the angle between a perpendicular line to the longitudinal axis of the first metatarsal and a line delineating the orientation of the metatarsal head articular surface (Fig. 2) [19]. The articular surface was identified by the subchondral sclerotic bone or the continuation of the articular curve. The first metatarsal protrusion distance was defined as the distance between the arcs of the bisecting lines of the first and second metatarsals from the common intersection of the two lines (Fig. 3) [9].
Fig. 1.

On the weightbearing dorsoplantar foot radiograph, angles between lines were measured. Various lines were drawn; line a is the longitudinal axis of the distal phalanx of the big toe, line b is the longitudinal axis of the proximal phalanx, line c is orientation of the proximal phalangeal base articular surface, line d is the longitudinal axis of the first metatarsal, line e is the longitudinal axis of the second metatarsal, line f is the longitudinal axis of the middle cuneiform, and line g is the longitudinal axis of the talus. Hallux valgus angle is the angle between b and d, intermetatarsal angle is the angle between d and e, interphalangeal angle is the angle between a and b, proximal phalangeal articular angle is the angle between b and c, and simplified metatarsus adductus angle is the angle between e and f.
Fig. 2.

The distal metatarsal articular angle (asterisk) is the angle between a perpendicular line to the longitudinal axis of the first metatarsal and a line delineating the orientation of the metatarsal head articular surface.
Fig. 3.

The first metatarsal protrusion distance is the difference between the arcs of the bisecting lines of the first (a) and second metatarsals (b) from the common intersection of the two lines.
One index was measured on the weightbearing sesamoid axial view. The sesamoid rotation angle was defined as the angular relationship between the weightbearing surface and a line connecting the most inferior aspect of the medial and lateral sesamoid [13] (Fig. 4).
Fig. 4.
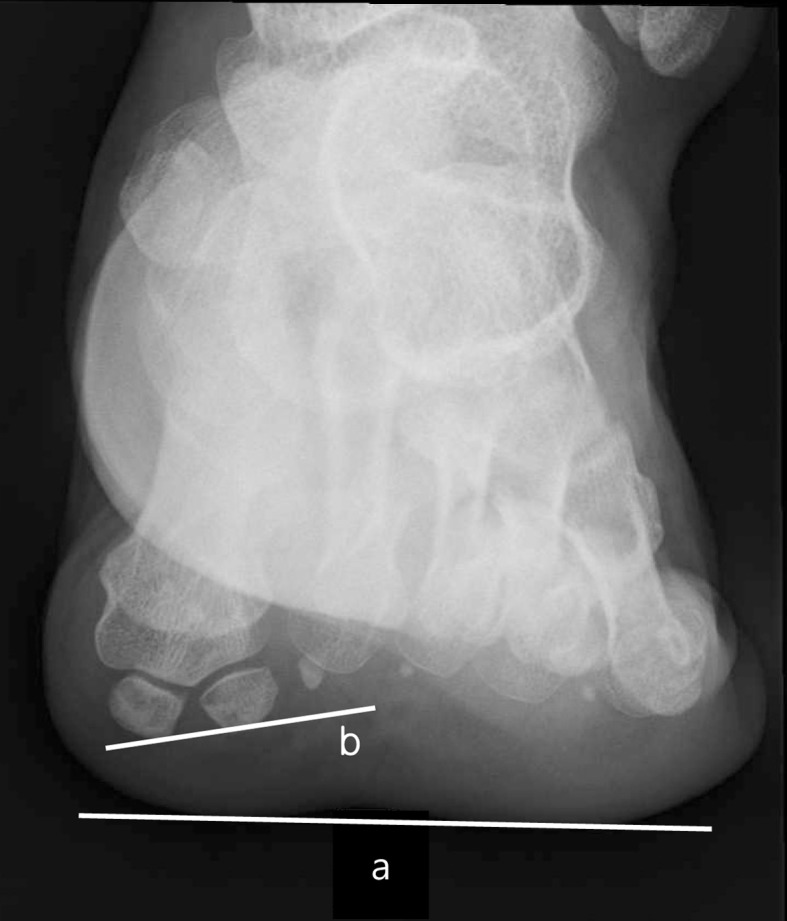
The sesamoid rotation angle is the angular relationship between the weightbearing surface and a line connecting the most inferior aspect of the medial and lateral sesamoid (angle between a and b).
To determine interobserver reliability we randomly selected 36 foot radiographs of 36 patients based on sample size calculation. The three orthopaedic surgeons (KML, KHS, TWK) measured the radiographic indices independently without knowledge of the patients’ clinical information and the other orthopaedic surgeons’ measurements. The order of the 36 radiographs was presented randomly to each orthopaedic surgeon by a research assistant using statistical software (SPSS, 15.0, Chicago, IL). To determine intraobserver reliability, one (KHS) of the three orthopaedic surgeons repeated the measurements for the 36 radiographs with an interval of 4 weeks. We analyzed the interobserver and intraobserver reliabilities using the ICCs; 95% CIs were determined in the setting of a two-way random effect model, a single measurement, and absolute agreement.
One author (KHS) measured the radiographic indices on all films, and the data were used for the correlation test and multiple regression analysis.
We used descriptive statistics to summarize the patients’ demographics and radiographic measurements. The data normality was determined using a Kolmogorov-Smirnov test. The correlations between the radiographic measurements were analyzed using Pearson’s correlation coefficients to investigate the relationships among the radiographic measurements on different planes. Multiple regression analysis was performed to examine the radiographic measurements predicting the hallux valgus angle after univariate analysis; variables at the p value of ≤ 0.1 in the univariate analysis were included in multiple regression. The goodness of fit was presented as the adjusted r2 value. Data from one author’s (KHS) measurements were used for correlation and multiple regression analyses.
Results
The hallux valgus angle had the highest interobserver reliability with an ICC of 0.985 (95% CI, 0.975–0.992) followed by the sesamoid rotation angle (ICC, 0.925; 95% CI, 0.875–0.958) and first metatarsal protrusion distance (ICC, 0.901; 95% CI, 0.836–0.943). The distal metatarsal articular angle had the lowest interobserver reliability with an ICC of 0.380 (95% CI, 0.149–0.592) followed by the simplified metatarsus adductus angle (ICC, 0.620; 95% CI, 0.452–0.760) (Table 2). In intraobserver reliability, the hallux valgus angle showed the highest ICC value (0.989; 95% CI, 0.979–0.994) and the simplified metatarsus adductus angle the lowest (0.756; 95% CI, 0.583–0.864), respectively (Table 3).
Table 2.
Interobserver reliabilities of radiographic measurements
| Reliability | HVA | IMA | IPA | DMAA | PPAA | Metatarsus adductus | First MT protrusion | SRA |
|---|---|---|---|---|---|---|---|---|
| ICC (95% CI) |
0.985 (0.975–0.992) |
0.896 (0.832–0.940) |
0.860 (0.777–0.919) |
0.380 (0.149–0.592) |
0.719 (0.579–0.829) |
0.620 (0.452–0.760) |
0.901 (0.836–0.943) |
0.925 (0.875–0.958) |
HVA = hallux valgus angle; IMA = intermetatarsal angle; IPA = interphalangeal angle; DMAA = distal metatarsal articular angle; PPAA = proximal phalangeal articular angle; Metatarsus adductus = simplified metatarsus adductus angle; First MT protrusion = first metatarsal protrusion distance; SRA = sesamoid rotation angle.
Table 3.
Intraobserver reliabilities of radiographic measurements
| Reliability | HVA | IMA | IPA | DMAA | PPAA | Metatarsus adductus | First MT protrusion | SRA |
|---|---|---|---|---|---|---|---|---|
| ICC (95% CI) |
0.989 (0.979–0.994) |
0.914 (0.841–0.954) |
0.884 (0.790–0.937) |
0.781 (0.622–0.878) |
0.819 (0.681–0.901) |
0.756 (0.583–0.864) |
0.944 (0.897–0.970) |
0.952 (0.909–0.975) |
HVA = hallux valgus angle; IMA = intermetatarsal angle; IPA = interphalangeal angle; DMAA = distal metatarsal articular angle; PPAA = proximal phalangeal articular angle; Metatarsus adductus = simplified metatarsus adductus angle; First MT protrusion = first metatarsal protrusion distance; SRA = sesamoid rotation angle.
The hallux valgus angle had the highest correlation with the distal metatarsal articular angle (r = 0.636, p < 0.001) followed by the intermetatarsal angle (r = 0.621, p < 0.001) and sesamoid rotation angle (r = 0.598, p < 0.001). The distal metatarsal articular angle had the highest correlation with the sesamoid rotation angle (r = 0.461, p < 0.001) (Table 4).
Table 4.
Correlation matrix of radiographic measurements
| Radiographic measurements | HVA | IMA | IPA | DMAA | PPAA | Metatarsus adductus | First MT protrusion |
|---|---|---|---|---|---|---|---|
| IMA | 0.620 (< 0.001) |
||||||
| IPA | −0.438 (0.001) |
−0.382 (< 0.001) |
|||||
| DMAA | 0.636 (< 0.001) |
0.467 (< 0.001) |
−0.323 (< 0.001) |
||||
| PPAA | −0.363 (0.001) |
−0.297 (< 0.001) |
0.284 (< 0.001) |
−0.284 (< 0.001) |
|||
| Metatarsus adductus | 0.112 (0.002) |
0.048 (0.197) |
0.072 (0.051) |
0.055 (0.134) |
0.001 (0.972) |
||
| First MT protrusion | 0.375 (< 0.001) |
0.196 (< 0.001) |
−0.113 (0.002) |
0.246 (< 0.001) |
−0.116 (0.002) |
0.256 (< 0.001) |
|
| SRA | 0.598 (< 0.001) |
0.470 (< 0.001) |
−0.348 (< 0.001) |
0.461 (< 0.001) |
−0.353 (< 0.001) |
−0.071 (0.060) |
0.203 (< 0.001) |
HVA = hallux valgus angle; IMA = intermetatarsal angle; IPA = interphalangeal angle; DMAA = distal metatarsal articular angle; PPAA = proximal phalangeal articular angle; Metatarsus adductus = simplified metatarsus adductus angle; First MT protrusion = first metatarsal protrusion distance; SRA = sesamoid rotation angle.
After univariate analysis, the intermetatarsal angle, interphalangeal angle, distal metatarsal articular angle, proximal phalangeal articular angle, first metatarsal protrusion distance, and sesamoid rotation angle were included in multiple regression analysis. Of these, intermetatarsal angle (p < 0.001), interphalangeal angle (p < 0.001), distal metatarsal articular angle (p < 0.001), first metatarsal protrusion distance (p < 0.001), sesamoid rotation angle (p < 0.001), and simplified metatarsus adductus angle (p = 0.009) were the measurements predicting hallux valgus angle (adjusted r2 = 0.632) (Table 5).
Table 5.
Multiple regression analysis to identify significantly contributing radiographic measurements to hallux valgus angle
| Radiographic measurements | Nonstandardized | Standardized beta | t-test | p value | |
|---|---|---|---|---|---|
| Beta | Standard error | ||||
| Coefficient | 5.798 | 1.508 | 3.845 | < 0.001 | |
| IMA | 0.794 | 0.085 | 0.265 | 9.325 | < 0.001 |
| IPA | −0.218 | 0.046 | −0.125 | −4.747 | < 0.001 |
| DMAA | 0.388 | 0.037 | 0.296 | 10.536 | < 0.001 |
| PPAA | −0.095 | 0.062 | −0.039 | −1.523 | 0.128 |
| Metatarsus adductus | 0.108 | 0.041 | 0.064 | 2.622 | 0.009 |
| First MT protrusion | 0.588 | 0.094 | 0.157 | 6.287 | < 0.001 |
| SRA | 0.212 | 0.024 | 0.251 | 8.694 | < 0.001 |
IMA = intermetatarsal angle; IPA = interphalangeal angle; DMAA = distal metatarsal articular angle; PPAA = proximal phalangeal articular angle; Metatarsus adductus = simplified metatarsus adductus angle; First MT protrusion = first metatarsal protrusion distance; SRA = sesamoid rotation angle.
Discussion
Various radiographic measurements have been developed and used for evaluating hallux valgus. However, some may not be necessary and their relationships have not been well established. We presumed determining their relationships could provide some insight into their usefulness. We therefore investigated the reliabilities of radiographic measurements and correlations among them and performed multiple regression analysis to determine which radiographic measurements predicted the hallux valgus angle.
Before discussing the findings of our study, study limitations need to be addressed. First, we studied only the relationships of the radiographic measurements and not the symptomatic correlation of the radiographic measurements or postoperative responsiveness as a result of the retrospective nature of the study. A longitudinal study is required investigating the clinical relevance of the radiographic measurements. Second, the hallux valgus angle was used as a gold standard and as a dependent variable in multiple regression analysis although hallux valgus is a complex three-dimensional deformity, and hallux valgus angle can explain the deformity on only one plane. However, hallux valgus deformity is defined and graded primarily by the hallux valgus angle observed on radiographs [4].
In this study, the hallux valgus angle had the highest ICC and most of the radiographic measurements had high ICC values greater than 0.8 on either interobserver or intraobserver reliability testing except for the distal metatarsal articular angle and simplified metatarsus adductus angle. The distal metatarsal articular angle and simplified metatarsus adductus angle had much lower ICC values compared with previous study results [3, 5, 15, 20, 21, 24] (Table 6). The ICC value of the simplified metatarsus adductus angle might have been affected by a narrow measurement range [22], and unclear landmarks for the distal metatarsal articular surface may have caused the relatively lower ICC values.
Table 6.
Reliabilities of radiographic indices measuring hallux valgus reported in previous studies
| Study | Year | Radiographic index | ICC |
|---|---|---|---|
| Bryant et al. [3] | 2000 | HVA | 0.96 (intraobserver) |
| IMA | 0.91 (intraobserver) | ||
| IPA | 0.88 (intraobserver) | ||
| First MT protrusion | 0.92 (intraobserver) | ||
| Menz and Munteanu [15] | 2005 | HVA | 0.99 (intraobserver) |
| 0.96 (interobserver) | |||
| IMA | 0.92 (intraobserver) | ||
| 0.87 (interobserver) | |||
| IPA | 0.87 (intraobserver) | ||
| 0.77 (interobserver) | |||
| Saro et al. [20] | 2005 | HVA | 0.97 (intraobserver) |
| 0.97 (interobserver) | |||
| Shima et al. [21] | 2009 | HVA | 0.91–0.99 (intraobserver) |
| 0.90–0.98 (interobserver) | |||
| IMA | 0.79–0.93 (intraobserver) | ||
| 0.78–0.94 (interobserver) | |||
| Srivastava et al. [24] | 2010 | HVA | 0.98–0.99 (intraobserver) |
| 0.97 (interobserver) | |||
| IMA | 0.98–0.99 (intraobserver) | ||
| 0.98 (interobserver) | |||
| IPA | 0.98–0.99 (intraobserver) | ||
| 0.99 (interobserver) | |||
| DMAA | 0.96–0.98 (intraobserver) | ||
| 0.96 (interobserver) | |||
| D’Arcangelo et al. [5] | 2010 | HVA | 0.95 (intraobserver) |
| IMA | 0.83 (intraobserver) | ||
| IPA | 0.66 (intraobserver) | ||
| DMAA | 0.90 (intraobserver) | ||
| PPAA | 0.73 (intraobserver) | ||
| First MT protrusion | 0.89 (intraobserver) | ||
| Metatarsus adductus | 0.88 (intraobserver) | ||
| Current study | 2012 | HVA | 0.989 (intraobserver) |
| 0.985 (interobserver) | |||
| IMA | 0.914 (intraobserver) | ||
| 0.896 (interobserver) | |||
| IPA | 0.884 (intraobserver) | ||
| 0.860 (interobserver) | |||
| DMAA | 0.781 (intraobserver) | ||
| 0.380 (interobserver) | |||
| PPAA | 0.819 (intraobserver) | ||
| 0.719 (interobserver) | |||
| First MT protrusion | 0.944 (intraobserver) | ||
| 0.901 (interobserver) | |||
| Metatarsus adductus | 0.756 (intraobserver) | ||
| 0.620 (interobserver) |
HVA = hallux valgus angle; IMA = intermetatarsal angle; IPA = interphalangeal angle; DMAA = distal metatarsal articular angle; PPAA = proximal phalangeal articular angle; First MT protrusion = first metatarsal protrusion distance; Metatarsus adductus = simplified metatarsus adductus angle.
The hallux valgus angle correlated with the distal metatarsal articular angle, intermetatarsal angle, and sesamoid rotation angle. This confirms the complex three-dimensional nature of hallux valgus deformity. In addition, the distal metatarsal articular angle correlated strongly with the sesamoid rotation angle. Considering the shape of the metatarsal head is more prominent volarly, pronation deformity of the first metatarsal bone might cause the lateral shift of a volarly prominent metatarsal articular surface. This might have finally resulted in the increased distal metatarsal articular angle. Therefore, an increased distal metatarsal articular angle might not be a true deformity of the dorsoplantar radiographic image but a secondary projection of a pronation deformity. This could be an error caused by evaluating a three-dimensional deformity with a two-dimensional tool. If that is true, the necessity of a chevron medial closing wedge osteotomy to correct the increased distal metatarsal articular angle needs to be reevaluated after the pronation deformity of the first metatarsal bone is corrected. However, there is insufficient evidence regarding this issue and additional investigation will be needed. Furthermore, the intermetatarsal angle correlated with the sesamoid rotation angle. From this correlation between radiographic measurements, we assumed valgus and pronation occur concurrently at the first tarsometatarsal joint. If this is true, the proximal metatarsal osteotomy should include a rotational component and reduce the intermetatarsal angle. We propose a cadaveric study to clarify this issue. A previous study reported that postoperative sesamoid position was important in the surgical outcome [17], and surgeons need to focus on the pronation deformity more in evaluating and treating hallux valgus deformity. The simplified metatarsus adductus angle had a relatively low correlation with the hallux valgus angle. This angle can be used to evaluate the relationship between the forefoot and the midfoot, and the simplified metatarsus adductus angle was a contributing factor to the hallux valgus angle. Although it has been reported that the planovalgus foot deformity is associated with the hallux valgus deformity [16], the clinical relevance of the simplified metatarsus adductus angle needs to be investigated further.
In multiple regression analysis, intermetatarsal angle, interphalangeal angle, distal metatarsal articular angle, simplified metatarsus adductus angle, first metatarsal protrusion distance, and sesamoid rotation angle predicted hallux valgus angle. Those measurements are important in predicting the three-dimensional hallux valgus deformity, and their clinical implications require further investigation in a future study.
The hallux valgus angle, intermetatarsal angle, interphalangeal angle, sesamoid rotation angle, and first metatarsal protrusion distance are worth measuring for a hallux valgus deformity considering their reliability and predicting the three-dimensional hallux valgus deformity.
Acknowledgments
We thank Mi Sun Ryu BS, Jaebong Lee MS, Tae Won Kim MD, and Young Jin Park MD, for data management, statistical support, and advice.
Footnotes
Each author certifies that he or she, or a member of their immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution has approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation was waived by the ethical committee due to the retrospective nature of the study.
References
- 1.Balding MG, Sorto LA., Jr Distal articular set angle: etiology and x-ray evaluation. J Am Podiatr Med Assoc. 1985;75:648–652. doi: 10.7547/87507315-75-12-648. [DOI] [PubMed] [Google Scholar]
- 2.Bonett DG. Sample size requirements for estimating intraclass correlations with desired precision. Stat Med. 2002;21:1331–1335. doi: 10.1002/sim.1108. [DOI] [PubMed] [Google Scholar]
- 3.Bryant A, Tinley P, Singer K. A comparison of radiographic measurements in normal, hallux valgus, and hallux limitus feet. J Foot Ankle Surg. 2000;39:39–43. doi: 10.1016/S1067-2516(00)80062-9. [DOI] [PubMed] [Google Scholar]
- 4.Coughlin MJ, Mann RA, Saltzman CL. Surgery of the Foot and Ankle. 8. Amsterdam, The Netherlands: Elsevier Health Sciences; 2006. [Google Scholar]
- 5.D’Arcangelo PR, Landorf KB, Munteanu SE, Zammit GV, Menz HB. Radiographic correlates of hallux valgus severity in older people. J Foot Ankle Res. 2010;3:20. doi: 10.1186/1757-1146-3-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Easley ME, Wiesel SW. Operative Techniques in Foot and Ankle Surgery. Philadelphia, PA: Lippincott Williams & Wilkins; 2010. [Google Scholar]
- 7.Engel E, Erlick N, Krems I. A simplified metatarsus adductus angle. J Am Podiatry Assoc. 1983;73:620–628. doi: 10.7547/87507315-73-12-620. [DOI] [PubMed] [Google Scholar]
- 8.Farsetti P, Weinstein SL, Ponseti IV. The long-term functional and radiographic outcomes of untreated and non-operatively treated metatarsus adductus. J Bone Joint Surg Am. 1994;76:257–265. doi: 10.2106/00004623-199402000-00014. [DOI] [PubMed] [Google Scholar]
- 9.Hardy RH, Clapham JC. Observation on hallux valgus: base on a controlled series. J Bone Joint Surg Br. 1951;33:376–391. doi: 10.1302/0301-620X.33B3.376. [DOI] [PubMed] [Google Scholar]
- 10.Hawkins FB, Mitchell CL, Hedrick DW. Correction of hallux valgus by metatarsal osteotomy. J Bone Joint Surg Am. 1945;27:387–394. [Google Scholar]
- 11.Jay RM. Pediatric Foot and Ankle Surgery. Philadelphia, PA: WB Saunders; 1999. [Google Scholar]
- 12.Judge MS, LaPointe S, Yu GV, Shook JE, Taylor RP. The effect of hallux abducto valgus surgery on the sesamoid apparatus position. J Am Podiatr Med Assoc. 1999;89:551–559. doi: 10.7547/87507315-89-11-551. [DOI] [PubMed] [Google Scholar]
- 13.Kuwano T, Nagamine R, Sakaki K, Urabe K, Iwamoto Y. New radiographic analysis of sesamoid rotation in hallux valgus: comparison with conventional evaluation methods. Foot Ankle Int. 2002;23:811–817. doi: 10.1177/107110070202300907. [DOI] [PubMed] [Google Scholar]
- 14.Lorimer DL, Neale D, French GJ. Neale’s Disorders of the Foot: Diagnosis and Management. London, UK: Churchill Livingstone; 2002. [Google Scholar]
- 15.Menz HB, Munteanu SE. Radiographic validation of the Manchester scale for the classification of hallux valgus deformity. Rheumatology (Oxford). 2005;44:1061–1066. doi: 10.1093/rheumatology/keh687. [DOI] [PubMed] [Google Scholar]
- 16.Nguyen US, Hillstrom HJ, Li W, Dufour AB, Kiel DP, Procter-Gray E, Gagnon MM, Hannan MT. Factors associated with hallux valgus in a population-based study of older women and men: the MOBILIZE Boston Study. Osteoarthritis Cartilage. 2010;18:41–46. doi: 10.1016/j.joca.2009.07.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Okuda R, Kinoshita M, Yasuda T, Jotoku T, Kitano N, Shima H. Postoperative incomplete reduction of the sesamoids as a risk factor for recurrence of hallux valgus. J Bone Joint Surg Am. 2009;91:1637–1645. doi: 10.2106/JBJS.H.00796. [DOI] [PubMed] [Google Scholar]
- 18.Park MS, Kim SJ, Chung CY, Choi IH, Lee SH, Lee KM. Statistical consideration for bilateral cases in orthopaedic research. J Bone Joint Surg Am. 2010;92:1732–1737. doi: 10.2106/JBJS.I.00724. [DOI] [PubMed] [Google Scholar]
- 19.Piggott H. The natural history of hallux valgus in adolescence and early adult life. J Bone Joint Surg Br. 1960;42:749–760. [Google Scholar]
- 20.Saro C, Johnson DN, Martinez De Aragon J, Lindgren U, Fellander-Tsai L. Reliability of radiological and cosmetic measurements in hallux valgus. Acta Radiol. 2005;46:843–851. doi: 10.1080/02841850500270852. [DOI] [PubMed] [Google Scholar]
- 21.Shima H, Okuda R, Yasuda T, Jotoku T, Kitano N, Kinoshita M. Radiographic measurements in patients with hallux valgus before and after proximal crescentic osteotomy. J Bone Joint Surg Am. 2009;91:1369–1376. doi: 10.2106/JBJS.H.00483. [DOI] [PubMed] [Google Scholar]
- 22.Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86:420–428. doi: 10.1037/0033-2909.86.2.420. [DOI] [PubMed] [Google Scholar]
- 23.Sorto LA, Jr, Balding MG, Weil LS, Smith SD. Hallux abductus interphalangeus: etiology, x-ray evaluation and treatment. J Am Podiatry Assoc. 1976;66:384–396. doi: 10.7547/87507315-66-6-384. [DOI] [PubMed] [Google Scholar]
- 24.Srivastava S, Chockalingam N, El Fakhri T. Radiographic angles in hallux valgus: comparison between manual and computer-assisted measurements. J Foot Ankle Surg. 2010;49:523–528. doi: 10.1053/j.jfas.2010.07.012. [DOI] [PubMed] [Google Scholar]
- 25.Yildirim Y, Cabukoglu C, Erol B, Esemenli T. Effect of metatarsophalangeal joint position on the reliability of the tangential sesamoid view in determining sesamoid position. Foot Ankle Int. 2005;26:247–250. doi: 10.1177/107110070502600311. [DOI] [PubMed] [Google Scholar]