

Abstract
Background:
Domestic violence is a major contributor to physical and mental ill health of the victim, and it is evident to some degree, in every society of the world.
Objectives:
1) To study perception about domestic violence in the study population. 2) To compare prevalence of domestic violence within the three subgroups of the study population (i.e. spouses of psychotic patients, spouses of non-psychiatric patients and hospital staff).
Materials and Methods:
A cross-sectional study was conducted among married men and women coming to Dhiraj General Hospital. Interviews were conducted using a semi-structured questionnaire. Inquiry was done about their perception regarding domestic violence, own experience any time in their life, and about the form of violence. Data was entered and analyzed using SPSS.
Results:
42.7% of study participants had never heard the words domestic violence. The overall prevalence of any form of violence in the study population as a whole was 32.3%. There was no significant difference found in the proportion of domestic violence among the three groups. The prevalence of physical, emotional, sexual and economic domestic violence was 16.3%, 25.3%, 2% and 11.3% respectively. Younger age group and female sex were significantly associated with the occurrence of domestic violence.
Conclusion:
Apart from the high prevalence of domestic violence in the present era, it is evident from the study that the participants’ perception about domestic violence was low. Efforts should be made to raise public consciousness and reporting of domestic violence and its attendant consequences.
Keywords: Domestic violence, India, perceptions, prevalence
Domestic violence (also called domestic abuse, spousal abuse, or intimate partner violence) often refers to violence of any type, e.g. physical, emotional, sexual and economic/financial, by a family member or one spouse against another, but can also include violence between concomitant and unmarried intimate partners. Domestic violence is a major contributor to the physical and mental ill health of the victim, and it is evident to some degree, in every society of the world.[1,2] Popular emphasis has tended to be on women as victims, however, with the rise of men's movements and rights, there is now advocacy for men victimized by women.[3] Studies have shown that male and female adolescents with psychiatric disorders were at a greater risk of being involved in an abusive adult relationship.[4] It has also been found surprisingly that three out of five ever married women of the reproductive age group, view wife-beating as justified in some situations.[5,6] Several general population surveys as well as clinic-based studies provide substantial evidence associating heavy drinking with violent behavior in general and intimate partner violence in particular.[7,8]
In the present study, we have made an effort to find out about the awareness of domestic violence in our study population of married individuals in addition to its prevalence, association with demographic characteristics and outcome. Attempt has also been made to find out differences in the prevalence of domestic violence in the spouses of patients suffering from psychotic illness, spouses of patients with non-psychiatric illness and general population (with reference to violence being more common in psychotic patients).[9] So the following study was undertaken with the objectives of – 1) To study perception about domestic violence in the study population and 2) To compare prevalence of domestic violence within the three subgroups of the study population (i.e. – Group A-Hospital staff, Group B-Spouses of non-psychiatric patients and Group C-Spouses of psychotic patients).
MATERIALS AND METHODS
Study design
This study was a cross-sectional hospital-based study
Source of subjects
The study covered both ever-married men and women, attending the Dhiraj General Hospital. Out of the total sample size, an equal number of participants were selected from three sources— 1) Hospital staff 2) Spouses of non-psychiatric patients and 3) Spouses of psychotic patients—in the Dhiraj General Hospital.
Sample size
The sample size was calculated based on the available estimated prevalence of domestic violence. Based on the prevalence of domestic violence (27%) from the pilot study, with a confidence level of 95% and absolute precision of 5, the samples required were: 303 participants. Three participants refused to participate thus, samples of 300 were obtained (i.e. sample of 100 participants from three groups).
Inclusion criteria
Ever-married subjects above 18 years of age
Subjects not having any psychiatric illness at present
Subjects not having serious medical illness at present.
Exclusion criteria
Subjects not willing to give written informed consent
Subjects below 18 years of age.
Interviews were conducted using a semi-structured questionnaire (Appendix I). Perception of the participants regarding domestic violence was studied on the basis of their response to a set of questions for four main variables of domestic violence (physical, emotional, sexual and economic). Participants were also asked whether their spouse had committed violence against them at any time in their life, and if experienced, then in what form, its outcome and whether reported to anyone. They were asked whether influence of alcohol was a contributor to their spouse perpetrating violence. In addition data on socio-demographic details of the participants were collected. The questionnaires were piloted to check appropriateness, clarity and flow of questions among 10 participants before the initiation of the study, and these participants were not included in the study.
The study protocol was approved by the local institutional review board at the Dhiraj General Hospital. Individual informed consent was obtained from all participants.
All the interviews were conducted in the local language by the research investigator. Interviews took place in a private place of the hospital to maintain privacy and confidentiality. Participants were assured of the confidentiality of their responses. To attain all these, care was taken to establish rapport with every participant prior to interviews. Women and men were interviewed by women and men investigators, respectively. Individual verbal informed consent was obtained from all participants by explaining the purpose of the study. The study was carried out during April 2010–May 2011.
Outcome variables
Four principal domestic violence outcome variables considered in our analysis were: physical violence, psychological violence, sexual violence and economic violence. They were determined by response to a set of questions for each outcome variable. If a woman/man (as a victim) gave a positive response to any of the questions in a set, it was considered as violence of that category. In addition, the fifth variable, i.e. any form of domestic violence was derived. If at least one of the four forms of domestic violence (physical and/or psychological and/or sexual and/or economic) was present, it was considered as the presence of any form of domestic violence. During logistic regression analyses, these outcome variables were dichotomized into presence and absence of violence, for each type of violence.
Data management and analysis
Data was entered into MS Excel sheet and exported to Epi Info (Version 3.5.1, developed by WHO CDC) and SPSS (15.0 version) and further analysis was carried out. Multivariate Logistic Regression was carried out to study association between occurrence of domestic violence (dependent variable) and demographic characteristics (independent variables) such as age, sex, education, occupation, income, religion, family type and domicile. The odds ratio (OR) is the value by which odds of the event (occurrence of violence) change when the independent variable increases by one unit/step. And it has been calculated by adjusting for all other independent variables in multivariate models. A P value of less than 0.05 was considered as the minimum level of significance.
RESULTS
Most of the study population/participants belonged to the 20-30 years’ age group (46.3%) and those from extremes of age groups (i.e.-<20 years and >50 years) were the least; 47.3% of participants were males and 52.7% were females. Participants were selected almost equal to avoid selection bias between the two groups and the majority of the participants were Hindu (85.7%). The majority of the participants (62%) had studied till school (i.e. either primary or secondary or higher secondary). Most of the participants (83.3%) were from middle socioeconomic status and 24.7% were from lower socioeconomic strata. Out of the total study population of 300 individuals, the majority (94.7%) was presently staying with spouse, 2.7% were divorced or separated and another 2.7% were widow/widower. Almost equal number of participants belonged to nuclear and joint family whereas half (53%) the participants were from the rural area.
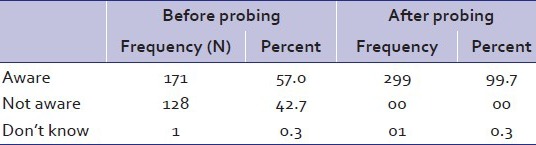
On asking the participants about their awareness pertaining to domestic violence, without probing them, 57% of the study population was aware about domestic violence and that it existed in society; 42.7% of the participants had never heard the words domestic violence. A major finding is that after introducing the subjects to the definition of domestic violence, almost all the participants, i.e.99.7% admitted that it existed in society [Table 1].
Table 1.
Awareness about existence of domestic violence before and after probing, among the study population
Out of the different acts of domestic violence, among the physical violence group, overburdening with work was considered as domestic violence by 65% of the population, which is the least perceived form in the physical violence group. Maximum number of participants (99.3%) considered an attempt to kill as domestic violence. Within the emotional violence subgroup, half the population studied believed - taunting, restricting freedom of choice, not giving equal opportunity, ignoring/indifference/not communicating, and deprivation of sexual relation – as domestic violence. As regards sexual violence, all the study participants considered pressure to go for prostitution and forced sexual relation with other family member as domestic violence, while 18.3% participants believed that forced sexual intercourse by spouse is not domestic violence. In the study population, for the items categorized as economic violence, maximum number of participants (84.0%) believed that demanding dowry is domestic violence, followed by act of taking away belongings (73.7%), followed by not providing sufficient finances (71.3%), followed by not allowing to have control over one's income (56.0%); the least number of participants believed that non-involvement in financial decisions is domestic violence (41.8%) [Table 2].
Table 2.
Perception about different acts as domestic violence among the study population

Among the four main variables of domestic violence, occurrence of physical violence was found to be 19.6%, emotional violence in 25.3%, financial violence in 11.3% and sexual violence in 2% of victims [Table 3].
Table 3.
Prevalence of overall and individual type of domestic violence in the three subgroups of study population

There was no significant difference found in the prevalence of domestic violence (neither overall nor in individual type) among the three subgroups of study participants, i.e. general population, spouses of non-psychiatric patients and spouses of psychotic patients [Table 3].
Some additional findings of our study were that among the participants who had experienced domestic violence, 41.2% had experienced it when the spouse was under the influence of alcohol.
Of the study population who had experienced domestic violence, 47.42% had never reported it or disclosed it to anyone. The most common reason for not reporting was fear of social stigma (in 63.4%). Among those who had reported, only 1.96% had reported it to the police, the remaining majority of the population had only shared it with relatives or friends.
Sixty-six percent of the population studied preferred to compromise with the situation, 14.4% left the house, 10.3% negotiated with the family members, 6.6% took help of community members for reconciliation, 2.1% retaliated (reciprocal domestic violence) and 1% took the help of the police.
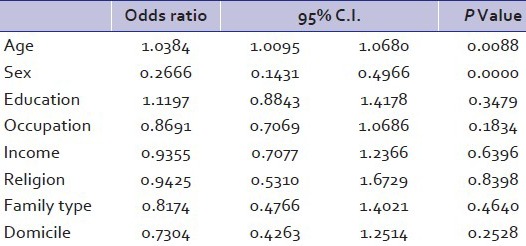
Out of the different demographic characteristics of the study population, the occurrence of domestic violence was significantly associated with the sex of the participants in the study group. The OR of occurrence of domestic violence in relation to the sex of the participant was 0.2666 (with 95% C.I. 0.1431-0.4966 and P value 0.0000), inferring that the female sex had highly significant association with occurrence of domestic violence [Table 4].
Table 4.
Association of various demographic details with the occurrence of domestic violence
Multivariate logistic regression
On applying multivariate logistic regression, the present study demonstrated that domestic violence is not significantly associated with age, domicile, education, occupation, family income, religion and type of family. Hence, prevalence of domestic violence was more common in females.
DISCUSSION
Violence against women is a major public health problem, which affects physical, mental and reproductive health.[10,11,12,13,14] Apart from the high prevalence of domestic violence in the present era, it is evident from the study that the participants’ perception/knowledge about domestic violence was rather low and a simple discussion in person easily helped the respondents identify domestic violence.
With regard to perception or awareness about domestic violence, findings were similar to that found in the National Family Health Survey (NFHS), where 41% of women thought that husbands were justified in slapping their wives if the latter showed disrespect to their in-laws, and a substantial 35% of women thought they deserved a brutal beating at the hands of their spouses if they neglected doing the household chores or looking after their children.[8] A study demonstrates that a large percentage of Nigerian women agreed that a man is justified in beating or hitting his wife; 66.4% and 50.4% of ever-married and unmarried women respectively expressed consent for wife-beating.[15]
The overall prevalence of domestic violence in our study population was found to be 32.3%. This is almost similar to the findings of many studies with 37–56% women reporting domestic violence in India.[8,16,17] In the present study we also found that domestic violence had a significant association with female gender and younger age. This was similar to the results of certain population-based studies.[16]
It is due to male patriarchy, which is defined as a system of male dominance legitimated within the family and the society through superior rights, privileges, authority and power.[18] No significant association was found with any of the other demographic characteristics of the study participants. Conversely, some community-based study from India observed that prevalence of domestic violence was more in women who were employed and in the lower socioeconomic strata.[19,20]
On comparing the prevalence of different forms of domestic violence in our findings to many population-based studies, the prevalence of physical violence was found to be the same, i.e. around 14–34% in other studies, while that of sexual and emotional violence was found to be less, i.e. prevalence of emotional violence was around 52% and sexual violence around 25%.[8,16] Hence domestic violence is a worldwide public health problem existing in all communities.[21,22,23]
Regarding alcohol influence among participants who experienced domestic violence, a similar inference was drawn from other studies which found that physical (44.86) and psychological (68.22%, P<0.001) abuse was significantly higher and sexual abuse was 10.28% in wives of alcohol-dependent males as compared to 28.4%, 27.10% and 4.67% respectively in wives of abstainers.[24]
The findings of the study refute once again the general myth in the community that psychotic patients are largely violent. Even though the National Commission for Women and the active role of state governments in publicizing the problems of Domestice violence, the study findings suggest that these have disseminated poorly. We would recommend to develop a better program to be developed for bringing about wider awareness in general population.
However, a larger sample size should be taken in order to have a proper idea about differences between the groups.
Appendices

Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.McCauley J, Kern DE, Kolodner K, Dill L, Schroeder AF, DeChant HK, et al. The “battering syndrome”: Prevalence and clinical characteristics of domestic violence in primary care internal medicine practices. Ann Intern Med. 1995;123:737–46. doi: 10.7326/0003-4819-123-10-199511150-00001. [DOI] [PubMed] [Google Scholar]
- 2.Roberts GL, Lawrence JM, O’Toole BI, Raphael B. Domestic violence in the emergency department: I: Two case-control studies of victims. Gen Hosp Psychiatry. 1997;19:5–11. doi: 10.1016/s0163-8343(96)00119-3. [DOI] [PubMed] [Google Scholar]
- 3.References Examining Assaults By Women On Their Spouses Or Male Partners: An Annotated Bibliography. [Last accessed on 2011 Sept 8]. Available from: http://www.csulb.edu/-mfiebert/assault.htm .
- 4.Ehrensaft MK, Moffitt TE, Caspi A. Is domestic violence followed by an increased risk of psychiatric disorders among women but not among men? A longitudinal cohort study. Am J Psychiatry. 2006;163:885–92. doi: 10.1176/ajp.2006.163.5.885. [DOI] [PubMed] [Google Scholar]
- 5.Sahoo, Harihar, Pradhan MR. New Delhi: INDE: Serials; 2009. Domestic Violence In India: An Empirical Analysis. [Google Scholar]
- 6.Hindin MJ. Understanding women's attitude towards wife beating in Zimbabwe. Bull World Health Organ. 2003;81:501–8. [PMC free article] [PubMed] [Google Scholar]
- 7.Fals-Stewart W. The occurrence of partner physical aggression on days of alcohol consumption: A longitudinal diary study. J Consult Clin Psychol. 2003;71:41–52. doi: 10.1037//0022-006x.71.1.41. [DOI] [PubMed] [Google Scholar]
- 8.National Family Health Survey III. 2005-2006;1(Chapter 15.4):507–20. [Google Scholar]
- 9.Mc Niel, Dale E. Correlates of violence in psychotic patients. Psychiatr Ann. 1997;27:683–9. [Google Scholar]
- 10.Garcia-Moreno C, Jansen HA, Ellsberg FM, M Heise L, Watts C. WHO multi-country study on women's health and domestic violence against women: Initial results on prevalence, health outcomes and women's responses. Bull World Health Organ WHO. 2005:5–10. [Google Scholar]
- 11.Mayhew S, Watts C. Cambridge: Cambridge University Press; 2002. Health policy in a globalising world. [Google Scholar]
- 12.Campbell J, Jones AS, Dienemann J, Kub J, Schollenberger J, O’Campo P, et al. Intimate partner violence and physical health consequences. Arch Intern Med. 2002;162:1157–63. doi: 10.1001/archinte.162.10.1157. [DOI] [PubMed] [Google Scholar]
- 13.Campbell JC. Health consequences of intimate partner violence. Lancet. 2002;359:1331–6. doi: 10.1016/S0140-6736(02)08336-8. [DOI] [PubMed] [Google Scholar]
- 14.Garcia-Moreno C, Heise L, Jansen HA, Ellsberg M, Watts C. Public health. Violence Against Women. Science. 2005;310:1282–3. doi: 10.1126/science.1121400. [DOI] [PubMed] [Google Scholar]
- 15.Oyediran KA, Isiugo-Abanihe U. Perceptions of Nigerian women on domestic violence: Evidence from 2003 Nigeria Demographic and Health Survey. Afr J Reprod Health. 2005;9:38–53. [PubMed] [Google Scholar]
- 16.Babu BV, Kar SK. Domestic violence against women in eastern India: A population-based study on prevalence and related issues. BMC Public Health. 2009;9:129. doi: 10.1186/1471-2458-9-129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chaudhary A, Girdhar S, Soni RK. Epidemiological correlates of married women in urban area of Ludhiana, Punjab, India. Internet J Health. 2009;9:9. [Google Scholar]
- 18.Krishnaraj M. Bombay: Research Centre for Women's Studies. Mumbai, India: SNDT Women's University; 1991. Women and violence – a country report. [Google Scholar]
- 19.Jeyaseelan L, Kumar S, Neelakantan N, Peedicayil A, Pillai R, Duvvury N. Physical Spousal Violence Against Women In India: Some Risk Factors. J Biosoc Sci. 2007;39:657–70. doi: 10.1017/S0021932007001836. [DOI] [PubMed] [Google Scholar]
- 20.Martin SL, Kilgallen B, Tsui AO, Maitra K, Singh KK, Kupper LL. Sexual Behaviors and Reproductive Health Outcomes. JAMA. 1999;282:1967–72. doi: 10.1001/jama.282.20.1967. [DOI] [PubMed] [Google Scholar]
- 21.Heise L, Ellsberg M, Gottmoeller M. A global overview of gender-based violence. Int J Gynaecol Obstet. 2002;78(Suppl 1):S5–14. doi: 10.1016/S0020-7292(02)00038-3. [DOI] [PubMed] [Google Scholar]
- 22.Martin SL, Tsui AO, Maitra K, Marinshaw R. Domestic violence in northern India. Am J Epidemiol. 1999;150:417–26. doi: 10.1093/oxfordjournals.aje.a010021. [DOI] [PubMed] [Google Scholar]
- 23.Garcia-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts CH. Prevalence of intimate partner violence: Findings from the WHO multi-country study on women's health and domestic violence. Lancet. 2006;368:1260–9. doi: 10.1016/S0140-6736(06)69523-8. [DOI] [PubMed] [Google Scholar]
- 24.Pinto VN. Comparative Study of Domestic Violence in Wives of Alcohol Dependent Males Versus That in Abstainers/Social Drinkers Wives. Bombay Hosp J. 2009;51:203–8. [Google Scholar]