
Figure 1.
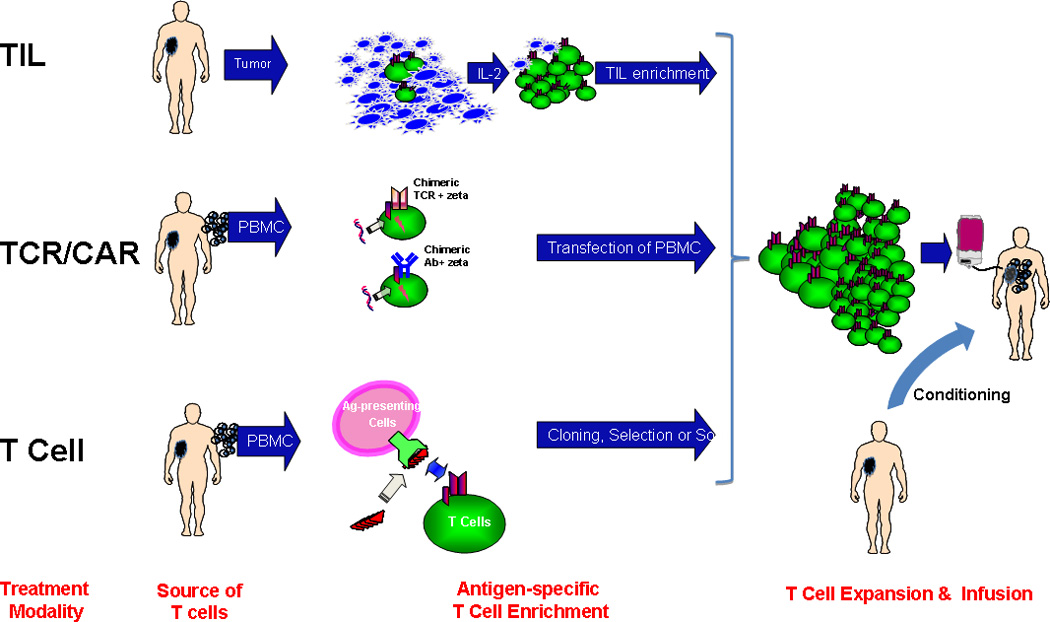
Adoptive Cell Therapy is represented by three general approaches:
- Enrichment and expansion of tumor-infiltrating lymphocytes (TIL) from a disaggregated tumor biopsy sample
- Genetic transfer of T Cell Receptor (TCR) recognizing tumor antigen-derived peptide-MHC target or Chimeric Antibody Receptor (CAR) recognizing surface tumor protein
- Enrichment of endogenous antigen-specific T cells from peripheral blood mononuclear cells by in vitro stimulation followed by cell selection or cloning. PBMCs are a source of both antigen-presenting cells and T cells.