
Figure 3.
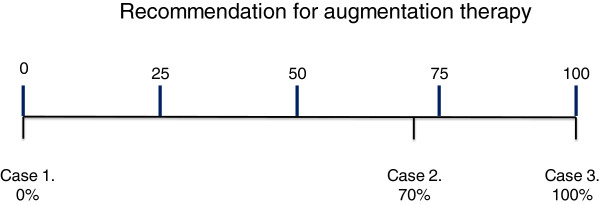
Recommendation for augmentation therapy. A new scale. Indications for augmentation therapy can vary from not to definitely indicated. Several factors will influence where the patient is placed on the scale including age, baseline lung function (FEV1 and/or Kco) and rate of decline expressed as a% predicted. A potential example is to divide the scale into quartiles with the lowest being age 60+ and/or lung function >80% predicted and/or decline < 0.1% predicted /year. The second quartile could be 50–60 years age and/or lung function 60-80% predicted and/or decline of 0.1-0.5% predicted /year. Third quartile 40–50 years age and/or lung function 40-60% predicted and/or decline of 0.5-1.0% predicted/year. Fourth quartile 30–40 years age and/or lung function 30-40% predicted and /or decline >1.0% predicted/year. This concept is summarised in Table 2. Footnote: Case 1. 75 years-old male, ex-smoker, or other non-index case with normal physiology. Indication for augmentation therapy 0% Case 2. 61 years-old male, exsmoker of 40 pack-years, index case. FEV1 = 58% predicted with KCO = 75% predicted. One ambulatory exacerbation the previous year. Previous spirometry one year ago FEV1 = 60% and 2 years ago = 62%. Indication for augmentation therapy 70%. Case 3. 42 years-old female, index case, exsmoker of 14 pack-years, FEV1 = 42% predicted and KCO = 32% predicted. Hospitalisation for exacerbation 5 months ago. Previous spirometry one year ago FEV1 = 51% predicted or patient with declining physiology despite smoking cessation and maximal usual therapy as in the patient in Figure 1 Indication for augmentation therapy 100%.