

Abstract
Purpose
Type of work might be related to insulin resistance and the metabolic syndrome (MetS). However, scant data are available. We performed this study to investigate whether the prevalence of MetS and insulin resistance differed according to occupation in middle-aged men.
Materials and Methods
In all, 2,348 men in their 40s~50s who had participated in the Korean National Health and Nutrition Examination Survey IV were included and were classified into two groups according to the type of work (manual worker vs. non-manual worker). Diagnosis of MetS required satisfying three or more of the National Cholesterol Education Program-Adult Treatment Panel III criteria. Fasting insulin, the glucose/insulin ratio (G/I ratio), and the homeostasis model assessment of insulin resistance (HOMA-IR) were used to estimate the insulin resistance. We used the Mann-Whitney test, χ2 tests, multiple linear regression test, and logistic regression analyses to examine the relationships.
Results
Age was significantly higher in the manual worker group. Body mass index was significantly lower in the manual worker group. Rates of current smoking and frequent drinking were higher in the manual worker group. In terms of surrogate markers of insulin resistance, the age-adjusted mean of fasting insulin, G/I ratio, and HOMA-IR indicated that lower insulin resistance was significantly related to manual work. After adjusting for age and other confounding factors, non-manual workers had a higher risk of the MetS than manual workers. The odds ratio in relation to MetS was significantly lower in the manual workers.
Conclusions
MetS and impaired insulin resistance are significantly related to non-manual work in middle-aged Korean men.
Keywords: Insulin resistance, Metabolic syndrome, Occupations
INTRODUCTION
The metabolic syndrome (MetS) is comprised of central obesity, dyslipidemia, hypertension, and glucose intolerance, although the definition of MetS varies according to ethnicity [1]. MetS is a risk factor for benign prostatic hyperplasia, type 2 diabetes mellitus, and coronary artery disease, and is associated with cerebrovascular disease and all-cause mortality [2,3].
MetS may be associated with lifestyle, and lifestyle modifications may be effective in resolving MetS and reducing the severity of related abnormalities in subjects with MetS [1]. The aforementioned issues indicate that the type of work a person does might be related to insulin resistance and MetS, considering that lifestyle is closely related to occupation. However, there are scant data concerning the relationship between type of work and insulin resistance and MetS in middle-aged men.
The evaluation of the relationship between type of work and MetS in middle-aged men might be important because MetS begins to occur in middle age and finding related factors might facilitate the establishment of a health policy on MetS in middle aged men [1].
Therefore, we undertook the present study using data from the Korean National Health and Nutrition Examination Survey (KNHANES) IV to investigate whether the prevalence of MetS and insulin resistance differed according to occupation in middle-aged men.
MATERIALS AND METHODS
1. Study subjects
Data from the KNHANES IV were used for this study. The KNHANES has been performed by the Korea Centers for Disease Control and Prevention to examine the general health and nutritional status of Koreans. To collect data representative of Koreans, they used a stratified three-stage clustered probability design (local district → enumeration district → household). Up to the present, four surveys have been completed as follows: I (1998), II (2001), III (2005), and IV (2007~2009). KNHANES IV enrolled 31,705 individuals. Among them, 24,871 individuals participated in the survey. To elucidate the relationship between the MetS and type of occupation in middle-aged men, the data of females, subjects less than 40 years old, and subjects more than 60 years old were excluded (Fig. 1). Cases missing data on MetS or occupation were also excluded. In the end, 2,348 men were included in this study.
Fig. 1.

Study flow diagram. KNHANES IV: the Korean National Health and Nutrition Examination Survey IV, MetS: metabolic syndrome.
The occupations were classified as manual work and non-manual work according to the Korean Standard Classification of Occupations. Service workers, managers, professionals, sales people, clerical workers, and professors were included in the non-manual workers. Simple labor work, agriculture, forestry, fishery, and manufacturing were included in manual work.
2. Metabolic syndrome assessment
Three blood pressure measurements (mmHg) were obtained 5 minutes apart with a mercury sphygmomanometer, and the last two measurements were averaged. The waist circumference (cm) was measured in the narrowest part between the lowest rib and the top of the hip. Body weight (kg) and body height (cm) were also measured. Blood samples were obtained with the subject in the fasting state for 12 hours and the insulin, glucose, triglycerides, and high-density lipoprotein cholesterol (HDL) were measured.
The diagnostic criteria for MetS had to satisfy three or more of the National Cholesterol Education Program-Adult Treatment Panel III criteria [4], as follows: 1) blood pressure ≥130/85 mmHg and/or antihypertensive medication; 2) fasting blood sugar ≥110 mg/dL and/or antidiabetic medication; 3) waist circumference ≥90 cm; 4) HDL cholesterol <40 mg/dL; and 5) triglycerides ≥150 mg/dL and/or antihypercholesterolemic medication.
3. Estimation of insulin resistance
Fasting insulin, the glucose/insulin ratio (G/I ratio), and the homeostasis model assessment of insulin resistance (HOMA-IR) were used to estimate insulin resistance [5]. The equations for the G/I ratio and HOMA-IR are as follows:
G/I ratio=glucose/insulin
HOMA-IR=(glucose×insulin)/405
In this study, the insulin concentration was reported in µU/mL and glucose in mg/dL.
4. Statistical analysis
The 2,348 men were classified into two groups according to the type of work (manual work vs. non-manual work). We compared the socio-demographic characteristics including age, body mass index (BMI), place of residence, income, education, marital status, smoking status, and drinking frequency of these two groups. The age-adjusted mean of components of the MetS, fasting insulin, G/I ratio, and HOMA-IR were also compared between the two groups. Finally, the odds ratio (OR) for type of work in relation to MetS was evaluated after adjusting for potential confounders (age, place of residence, type of home, individual income, education, marital status, smoking status, and drinking frequency).
Statistical analyses were performed with the t-test, χ2 tests, multiple linear regression test, and logistic regression analyses, using the SPSS version 11.0 (SPSS Inc., Chicago, IL, USA). p<0.05 was considered statistically significant.
RESULTS
1. Patient characteristics
Table 1 shows the characteristics of the subjects in this study. Age was significantly higher in the manual worker group. At the same time, body weight and BMI were significantly lower in the manual worker group. However, the rate of current smoking and frequent drinking (≥4 time/week) was higher in the manual worker group. The percentage of residence in a rural area, living in an apartment, very high individual income, and college education was higher in the non-manual worker group. There was no significant difference in marital status.
Table 1.
Socio-demographic characteristics
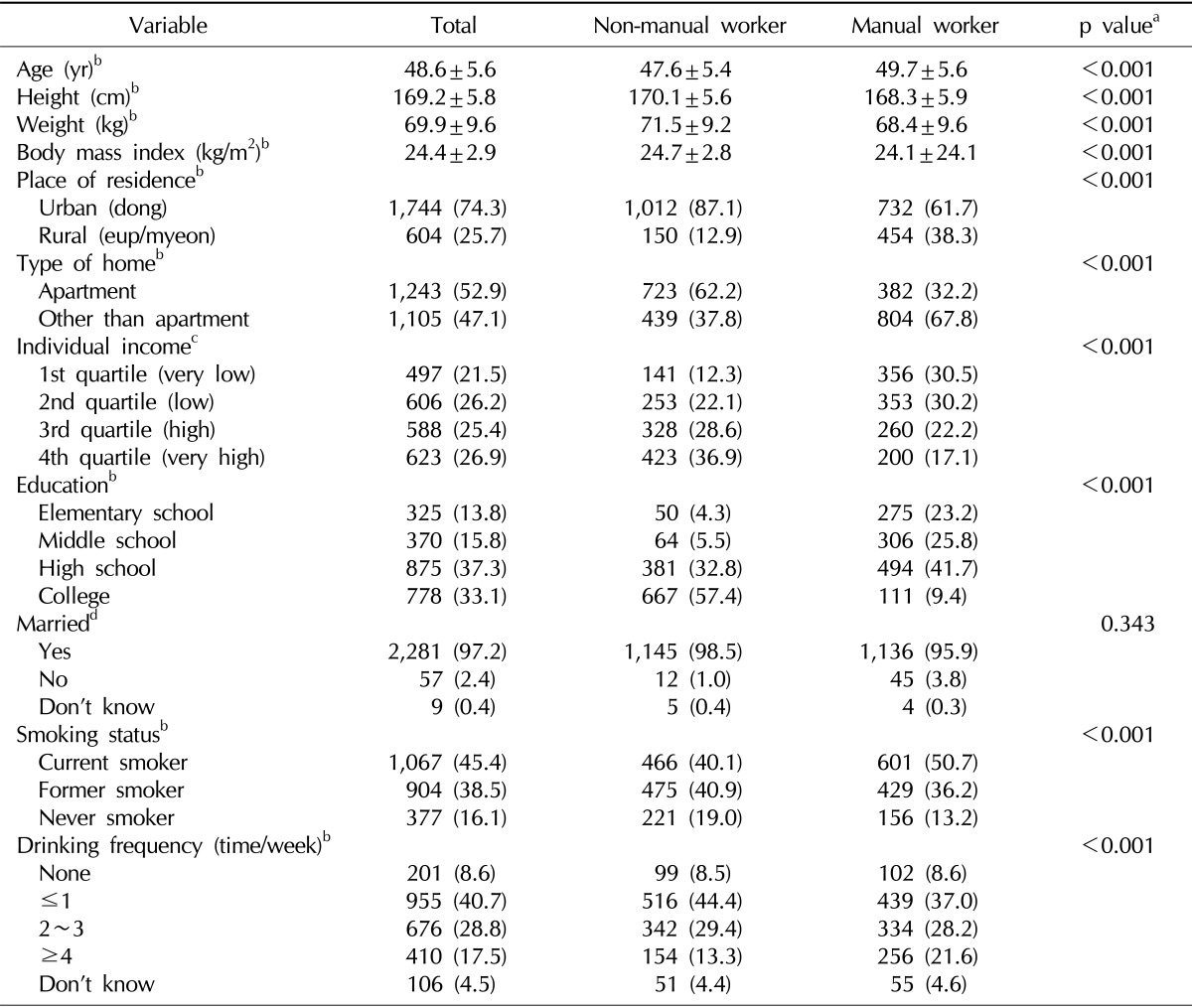
Values are presented as mean±standard deviation or number (%).
aChi-squared test or t-test. bn=2,348, cn=2,314, dn=2,347.
2. Comparison of components of metabolic syndrome and surrogate markers of insulin resistance between manual and non-manual workers
The prevalence of MetS was 25.0% in the manual workers and 27.7% in the non-manual workers. After adjusting for age, systolic blood pressure was significantly higher in the manual group (Table 2). However, the manual worker group had better values for the other components of the MetS; that is, the waist circumference of the manual workers was significantly lower than that of the non-manual workers, and the HDL of the manual workers was significantly higher than that of the non-manual workers. In terms of surrogate makers of insulin resistance, all of the parameters including fasting insulin, the G/I ratio, and HOMA-IR indicated that there was significantly lower insulin resistance in the manual workers. Additionally, the mean number of components of Mets was significantly higher in the non-manual workers.
Table 2.
Age-adjusted mean of components of metabolic syndrome, fasting insulin, HOMA-IR, and G/I ratio according to type of work
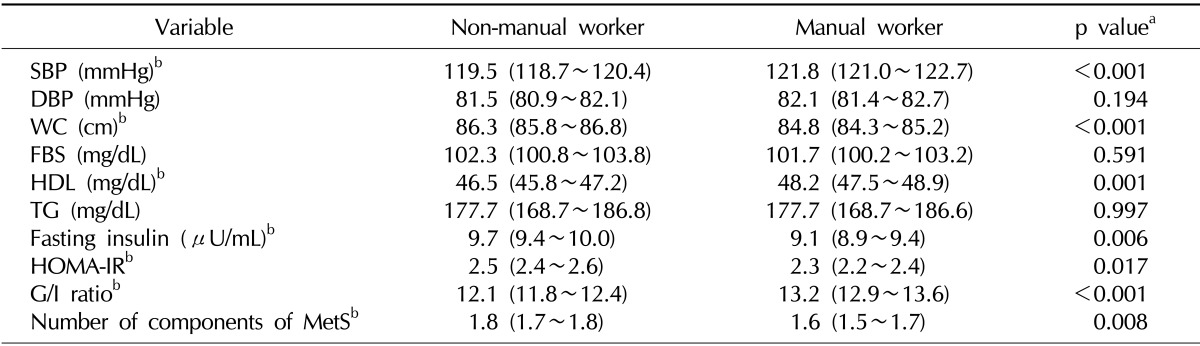
Values are presented as an age-adjusted mean (95% confidence interval).
HOMA-IR: homeostasis model assessment of insulin resistance, G/I ratio: glucose-insulin ratio, SBP: systolic blood pressure, DBP: diastolic blood pressure, WC: waist circumference, FBS: fasting blood sugar, HDL: high-density lipoprotein cholesterol, TG: triglyceride, MetS: metabolic syndrome.
aMultiple linear regression test: adjusted for age. bStatistically significant.
3. Odds ratio for metabolic syndrome in relation to type of work
After adjusting for age, the non-manual workers had a higher risk of the MetS than manual workers; that is, the OR in relation to MetS was significantly lower in the manual workers (Table 3). Furthermore, the significant difference in OR by the type of work in relation to MetS was maintained when controlling for other potential confounding factors (place of residence, type of home, individual income, education, marital status, smoking status, and drinking frequency).
Table 3.
Odds ratio for type of work in relation to metabolic syndrome
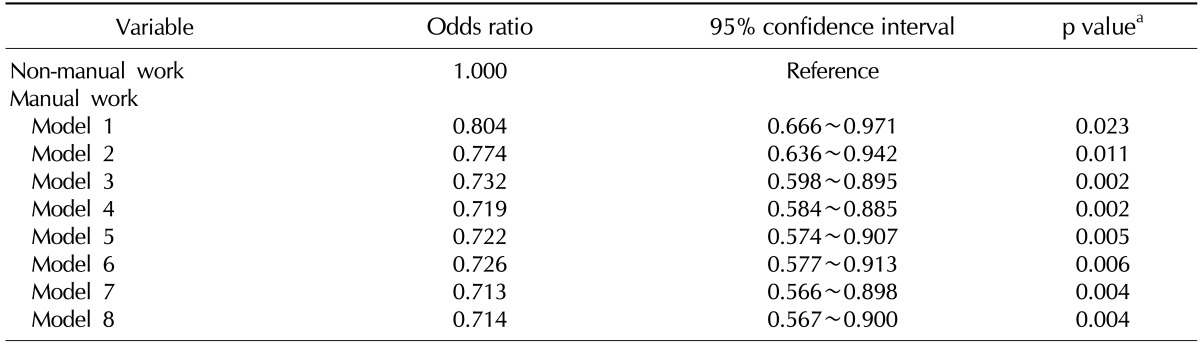
Odds ratios are listed with 95% confidence intervals with non-manual work as the reference category.
Model 1: adjusted for age; Model 2: adjusted for age and place of residence; Model 3: adjusted for age, place of residence, and type of home; Model 4: adjusted for age, place of residence, type of home, and individual income; Model 5: adjusted for age, place of residence, type of home, individual income, and education; Model 6: adjusted for age, place of residence, type of home, individual income, education, and marital status; Model 7: adjusted for age, place of residence, type of home, individual income, education, marital status, and smoking status; Model 8: adjusted for age, place of residence, type of home, individual income, education, marital status, smoking status, and drinking frequency.
aLogistic regression analysis.
DISCUSSION
The aim of this study was to evaluate the relationship between type of work and both insulin resistance and MetS in middle-aged Korean men. To our knowledge, this is the first study to estimate insulin resistance (fasting insulin, G/I ratio, and HOMA-IR) in middle-aged men and examine the relationship between type of work and MetS. Our data suggest that manual work is related to a lower prevalence of MetS and lower insulin resistance compared to non-manual work.
A few studies have demonstrated the effect of occupation on the prevalence of the MetS, but no data has been reported specifically concerning the relationship between occupation and MetS in middle-aged men. A cross-sectional study conducted in Spain demonstrated that the age-adjusted prevalence of the MetS in men was similar in blue-and white-collar workers [6]. However, a Korean cross-sectional study [7] reported that the rate of MetS in men (>50 years old) was significantly higher in non-manual workers than manual workers (43.3% vs. 31.9%). In our study, the rate of MetS was 25.0% in the manual workers and 27.7% in the non-manual workers. Without adjusting for age, the prevalence of MetS was non-significantly higher in the non-manual worker group. However, after adjusting for age, a logistic regression analysis indicated that the prevalence of MetS was significantly higher in the non-manual worker group. This difference is likely related to the difference in the average age between the two groups (Table 1). Additionally, the OR of MetS was significantly lower in the manual workers than the non-manual workers after adjusting for potential confounding factors. The previous Spanish data did not classify the MetS prevalence according to age. We think that this is responsible for those results being inconsistent with our data and previous Korean data. Therefore, it can be concluded that non-manual work may be associated with MetS in middle-aged Korean men.
Insulin resistance has been defined as a status in which more insulin is needed to maintain a normal serum glucose level [5]. Insulin resistance is known to be related to the pathophysiology of type 2 diabetes and is a hallmark of the MetS [8,9]. There are various methods for measuring insulin resistance [5]. Fasting insulin is known to detect insulin resistance before clinical disease appears [10]. It was also reported that the G/I ratio is a highly sensitive and specific measurement of insulin sensitivity [5]. HOMA-IR is another model of the relationship between glucose and insulin dynamics that predicts the fasting steady state glucose and insulin concentrations for a wide range of possible combinations of insulin resistance and β-cell function [5]. In this study, all of the aforementioned parameters indicated that manual work is related to significantly lower insulin resistance. This result is more evidence that manual work has a lower association with MetS than non-manual work.
In this study, the manual workers consumed more tobacco and alcohol than the non-manual workers. It is well known that smoking and alcohol are directly correlated with hypertension [11]. The aforementioned issue might explain why the systolic blood pressure was significantly higher in the manual workers. In terms of MetS, the impact of alcohol consumption on MetS remains uncertain, as the effect has not been consistent across several studies [12-17]. However, it has been reported that smoking is related to MetS and increases the risk of MetS [18-21]. Nevertheless, the OR for MetS was lower in the manual workers. Smoking might lead to visceral fat accumulation and insulin resistance, and it increases the risk of MetS [21]. However, all of the parameters of obesity (body weight, BMI, and waist circumference) of the non-manual workers were higher than those of the manual workers. The impact of smoking on MetS might have disappeared due to weight reduction through physical activity involved in manual work. These issues would explain the relationship of non-manual work with a lower rate of MetS even though the manual workers consumed more tobacco. Our results suggest that clinical attention and health policy for weight control and MetS are necessary in non-manual workers. Additionally, education about smoking and alcohol is necessary for manual workers.
In our study, to elucidate the role of age, place of residence, type of home, individual income, education, marital status, smoking status, and drinking frequency in relation to MetS and the type of occupation, we calculated the correlation after adjusting for these parameters in that order. After adjusting for these parameters, very little change occurred in the beta and p value for multiple linear regression. Therefore, the role of these parameters seems to have been limited in the relationship between lower urinary tract symptoms/benign prostatic hyperplasia and MetS and the type of occupation. We believe that further clinical data are needed to elucidate the role of these parameters in MetS and the type of work.
Several limitations of the present study warrant mention. First, the cross-sectional nature of the dataset makes causal inferences problematic. Second, we simply analyzed occupation as manual work and non-manual work; thus a potential bias may have occurred. Third, we did not adjust the physical activity factor in evaluating the relationship between MetS and the type of work because of very complex and segmented raw data on physical activity. This might be an important factor in their relationship. We believe that further clinical data are needed to elucidate the role of physical activity. Nevertheless, we think that our study is meaningful since this is the first study to elucidate an association between the type of work and insulin resistance, and it is the first study to elucidate an association between type of work and MetS in middle-aged men.
CONCLUSIONS
MetS and impaired insulin resistance are significantly related to non-manual work as compared to manual work in middle-aged Korean men. The results of this study may be helpful in establishing an effective health policy for middle-aged workers in Korea.
References
- 1.Yamaoka K, Tango T. Effects of lifestyle modification on metabolic syndrome: a systematic review and meta-analysis. BMC Med. 2012;10:138. doi: 10.1186/1741-7015-10-138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hamaguchi M, Kojima T, Ohbora A, Takeda N, Fukui M, Kato T. Protective effect of alcohol consumption for fatty liver but not metabolic syndrome. World J Gastroenterol. 2012;18:156–167. doi: 10.3748/wjg.v18.i2.156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Park YW, Min SK, Lee JH. Relationship between lower urinary tract symptoms/benign prostatic hyperplasia and metabolic syndrome in Korean men. World J Mens Health. 2012;30:183–188. doi: 10.5534/wjmh.2012.30.3.183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. American Heart Association; National Heart, Lung, and Blood Institute. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112:2735–2752. doi: 10.1161/CIRCULATIONAHA.105.169404. [DOI] [PubMed] [Google Scholar]
- 5.Singh B, Saxena A. Surrogate markers of insulin resistance: a review. World J Diabetes. 2010;1:36–47. doi: 10.4239/wjd.v1.i2.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sánchez-Chaparro MA, Calvo-Bonacho E, González-Quintela A, Fernández-Labandera C, Cabrera M, Sáinz JC, et al. Ibermutuamur Cardiovascular Risk Assessment (ICARIA) Study Group. Occupation-related differences in the prevalence of metabolic syndrome. Diabetes Care. 2008;31:1884–1885. doi: 10.2337/dc08-0431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Myong JP, Kim HR, Jung-Choi K, Baker D, Choi B. Disparities of metabolic syndrome prevalence by age, gender and occupation among Korean adult workers. Ind Health. 2012;50:115–122. doi: 10.2486/indhealth.ms1328. [DOI] [PubMed] [Google Scholar]
- 8.Grundy SM, Brewer HB, Jr, Cleeman JI, Smith SC, Jr, Lenfant C, American Heart Association. National Heart, Lung, and Blood Institute Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation. 2004;109:433–438. doi: 10.1161/01.CIR.0000111245.75752.C6. [DOI] [PubMed] [Google Scholar]
- 9.Olefsky JM, Saltiel AR. PPAR gamma and the treatment of insulin resistance. Trends Endocrinol Metab. 2000;11:362–368. doi: 10.1016/s1043-2760(00)00306-4. [DOI] [PubMed] [Google Scholar]
- 10.American Diabetes Association. Consensus Development Conference on Insulin Resistance. 5-6 November 1997. Diabetes Care. 1998;21:310–314. doi: 10.2337/diacare.21.2.310. [DOI] [PubMed] [Google Scholar]
- 11.Slama M, Susic D, Frohlich ED. Prevention of hypertension. Curr Opin Cardiol. 2002;17:531–536. doi: 10.1097/00001573-200209000-00014. [DOI] [PubMed] [Google Scholar]
- 12.Baik I, Shin C. Prospective study of alcohol consumption and metabolic syndrome. Am J Clin Nutr. 2008;87:1455–1463. doi: 10.1093/ajcn/87.5.1455. [DOI] [PubMed] [Google Scholar]
- 13.Yokoyama H, Hiroshi H, Ohgo H, Hibi T, Saito I. Effects of excessive ethanol consumption on the diagnosis of the metabolic syndrome using its clinical diagnostic criteria. Intern Med. 2007;46:1345–1352. doi: 10.2169/internalmedicine.46.6196. [DOI] [PubMed] [Google Scholar]
- 14.Rosell M, De Faire U, Hellénius ML. Low prevalence of the metabolic syndrome in wine drinkers--is it the alcohol beverage or the lifestyle. Eur J Clin Nutr. 2003;57:227–234. doi: 10.1038/sj.ejcn.1601548. [DOI] [PubMed] [Google Scholar]
- 15.Gigleux I, Gagnon J, St-Pierre A, Cantin B, Dagenais GR, Meyer F, et al. Moderate alcohol consumption is more cardioprotective in men with the metabolic syndrome. J Nutr. 2006;136:3027–3032. doi: 10.1093/jn/136.12.3027. [DOI] [PubMed] [Google Scholar]
- 16.Djoussé L, Arnett DK, Eckfeldt JH, Province MA, Singer MR, Ellison RC. Alcohol consumption and metabolic syndrome: does the type of beverage matter? Obes Res. 2004;12:1375–1385. doi: 10.1038/oby.2004.174. [DOI] [PubMed] [Google Scholar]
- 17.Freiberg MS, Cabral HJ, Heeren TC, Vasan RS, Curtis Ellison R Third National Health and Nutrition Examination Survey. Alcohol consumption and the prevalence of the Metabolic Syndrome in the US.: a cross-sectional analysis of data from the Third National Health and Nutrition Examination Survey. Diabetes Care. 2004;27:2954–2959. doi: 10.2337/diacare.27.12.2954. [DOI] [PubMed] [Google Scholar]
- 18.Nakanishi N, Takatorige T, Suzuki K. Cigarette smoking and the risk of the metabolic syndrome in middle-aged Japanese male office workers. Ind Health. 2005;43:295–301. doi: 10.2486/indhealth.43.295. [DOI] [PubMed] [Google Scholar]
- 19.Miyatake N, Wada J, Kawasaki Y, Nishii K, Makino H, Numata T. Relationship between metabolic syndrome and cigarette smoking in the Japanese population. Intern Med. 2006;45:1039–1043. doi: 10.2169/internalmedicine.45.1850. [DOI] [PubMed] [Google Scholar]
- 20.Geslain-Biquez C, Vol S, Tichet J, Caradec A, D'Hour A, Balkau B D.E.S.I.R. Study Group. The metabolic syndrome in smokers. The D.E.S.I.R. study. Diabetes Metab. 2003;29:226–234. doi: 10.1016/s1262-3636(07)70031-9. [DOI] [PubMed] [Google Scholar]
- 21.Cena H, Fonte ML, Turconi G. Relationship between smoking and metabolic syndrome. Nutr Rev. 2011;69:745–753. doi: 10.1111/j.1753-4887.2011.00446.x. [DOI] [PubMed] [Google Scholar]