
Figure 5.
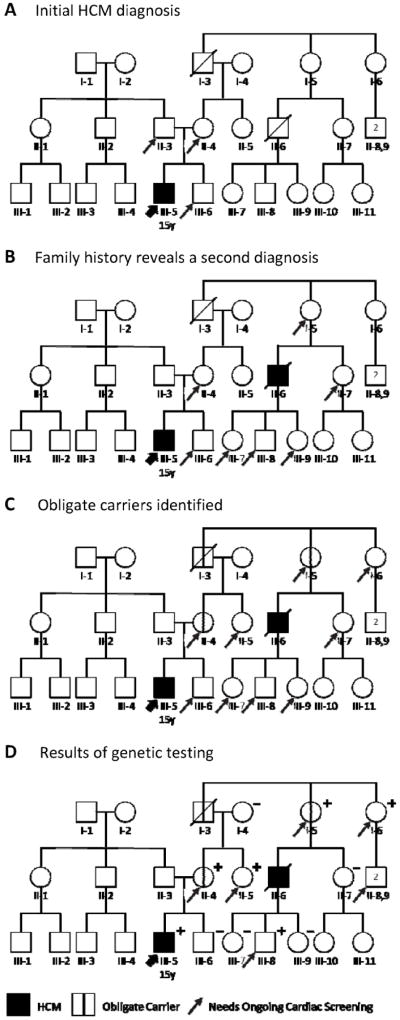
An evolving HCM family history, and careful pedigree assessment, shifts cardiology screening needs. A, Relatives needing screening based on initial diagnosis. Diagnosis of this 15-year-old patient (III-5, thick arrow) with HCM means his first-degree relatives (father II-3, mother II-4, and brother III-6; thin arrows) are each at 50% risk. B, Relatives needing screening based on initial plus a second diagnosis. When a second HCM diagnosis (II-6) is discovered in the patient’s maternal family history, this individual’s first-degree relatives (I-5, II-7, III-7, III-8, and III-9) also require cardiac screening. The patient’s father (II-3), not on the affected side of the family, is no longer considered at risk. C, Additional relatives need screening based on obligate carriers. Pedigree analysis identifies three obligate carriers (I-3, I-5, and II-4; marked with vertical line) connecting the individuals with HCM, including the patient’s mother. Each is at known risk for disease. Immediate family members of an obligate carrier are at 50% risk and also require screening (arrows added to I-6 and II-5). D, Genetic testing helps target screening to relatives definitively predisposed to HCM. In this family, several family members at 50% risk (II-7, III-6, III-7, and III-9) did not inherit the disease-causing variant; they and their descendants can be excused from further screening. By contrast, II-5 and I-6 test positive, newly revealing their children (II-8,9) to be at 50% risk. Circles indicate females; squares, males; slash, deceased; +, genetic variant present; –, genetic variant absent. HCM = hypertrophic cardiomyopathy. Adapted with permission from Ho.50