

Abstract
Background:
Allergic rhinitis (AR) is a highly prevalent allergic disease and also counts among the 10 most frequent reasons for medical consultation. Its impact on quality of life (QoL) and work productivity has been established but comparisons with other diseases are rare in the literature. The aim of this study was to evaluate the impact of AR in health-related QoL (HRQoL) and work productivity in primary care patients, compared with other prevalent diseases such as hypertension, diabetes mellitus (DM) type II, and symptomatic depression.
Methods:
Six hundred sixteen patients were included in a multicenter cross-sectional observational study. A generic HRQoL questionnaire, 36-item Short Form, and a specific questionnaire, “Work Productivity and Activity Impairment” were handed out to measure QoL and work productivity impact of the diseases. To assess clinical severity with a comparable scale between diseases Clinical Global Impression (CGI) had been used.
Results:
Symptomatic depression was found to produce the greatest impairment on work productivity with a decrease of 59.5%, with significant differences compared with AR, hypertension, and DM type II (p < 0.05). Symptomatic depression was found to produce the highest negative impact on daily activities with a statistically significant reduction of 59.4% (p < 0.05) compared with AR (26.6% decrease), hypertension (8.8% decrease), and DM (16.7% decrease) patients. Differences between AR and DM or hypertension were also significant (p < 0.05). Restriction on daily activities for AR was 27.8%, which is significantly higher (p < 0.05) than hypertension (19.8% decrease) but not DM (25.7% decrease). Depression had the highest impairment on daily activities (59.4%), compared with the remaining three groups (p < 0.05).
Conclusion:
AR impairs work productivity in a greater magnitude than hypertension and DM type II.
Keywords: Allergic rhinitis, clinical global impression scale, depression, diabetes mellitus type II, hypertension, quality of life, SF-36, restriction on daily activities, work productivity and activity impairment
Allergic rhinitis (AR) is a global health problem affecting 5–50% of the population and its prevalence is increasing.1 In our community 21% of people are affected.2 It is not only the most frequent allergic disease but also counts among the 10 most frequent reasons for medical consultation, generating an important economic impact.3,4 Although AR is not a severe disease, it has been acknowledged to have great impact of on quality of life (QoL), impairments in social life and productivity at school and work,5–7 and implies elevated social costs.8,9
In the last 10 years an increasing effort has been made to understand the socioeconomic burden of AR in terms of work productivity revealing important results, particularly in developed and western countries.1,10,11 AR, together with depression, is one of the first causes of work absenteeism, particularly during spring season.12 It is estimated that 1 of 10 workers suffer from AR; moreover, up to 70% of affected patients are unaware of negative effects of the disease.13 Loss of work productivity is a major problem because although employees attend their workplaces, there is an important impairment due to the disease known as “presenteeism.”14 This relationship has also been established in a study among primary care patients, which was developed in France.15 However, studies comparing AR with other diseases in terms of usual clinical practice are lacking.
The aim of the study was to evaluate the impact of AR in health-related QoL (HRQoL) and work productivity among primary care patients, compared with other prevalent diseases such as hypertension, diabetes mellitus (DM) type II, and symptomatic depression.
METHODS
A cross-sectional multicenter study was developed in 74 primary care centers, randomly selected nationwide. Patients were managed according to usual clinical practice and all variables were collected in one visit according to daily practice. Patients were recruited from March 15 to September 30, 2005.
Patients
Inclusion criteria were the following: (1) to be >18 years old and (2) to have been diagnosed with one of the four diseases considered in the study and mentioned previously. Exclusion criteria were to have a temporary disability and to suffer from more than one of the diseases evaluated in the study. Informed consent was obtained and the Hospital Ramón y Cajal (Madrid) Ethics Committee approved this study.
Study Design
In a unique visit the physician/researcher recruited the patient after informed consent and questionnaires were completed subsequently. Patients who suffered from one of the diseases included in the study were subsequently selected either until the end of the recruitment period or after fulfilling the intended number of patients.
Assessment of Diagnosis and Severity of the Diseases
A validated generic unique scale, viz., Clinical Global Impression (CGI), was used to measure the severity of the four diseases.16 This is a 7-point scale ranging from 1 to 7: 1, normal; 2, very mild; 3, mild; 4, moderate; 5, markedly; 6, severe; and 7, extremely severe.
The following subsections list the inclusion criteria for each disease considered in the study.
Allergic Rhinitis.
(1) Onset of symptoms at least 2 years ago, (2) diagnosis based on criteria proposed in the International Consensus of Rhinitis17 and the presence of IgE shown by skin-prick test and/or IgE in serum measured by using the CAP System FEIA (Phadia, Uppsala, Sweden) or seasonal AR symptoms at least for 2 years in the same seasonal period, and (3) a minimum score of 2 points in the total symptoms score (TSS5). TSS5 is a widely used and accepted instrument in AR clinical trials18 where nasal symptoms (blocked nose, runny nose, nose itch, sneeze, and itchy eyes) are scored from 0 to 3 (0, no symptoms; 1, mild; 2, moderate; and 3, severe) resulting in total score ranging from 0 (absence of symptoms) to 12 (maximum intensity of symptoms). A visual analog scale was also used in AR patients.19
Symptomatic Depression.
Patients diagnosed with depression with a score of ≥3 in the CGI Scale.20 Following World Health Organization recommendations, symptomatic depression is defined as a disorder that presents with depressed mood, loss of interest or pleasure, feelings of guilt or low self-worth, disturbed sleep or appetite, low energy, and poor concentration for a long period of time.21
Uncontrolled Hypertension.
Patients were diagnosed with hypertension if they had a systolic blood pressure over 140 mmHg and/or diastolic blood pressure over 95 mmHg on the day of their visit.
DM type II.
Patients were diagnosed with DM type II following current World Health Organization diagnostic criteria defined as fasting plasma glucose of ≥7.0 mmol/L (126 mg/dL) or 2 hours of plasma glucose of ≥11.1 mmol/L (200 mg/dL) plus symptoms of DM (polyuria, polydipsia, or unexplained weight loss).22 Patients suffering from two or more diseases of the aforementioned list were excluded.
Data Analysis
Demographic characteristics—sex, age, type of job (physical, intellectual, or both), comorbidity (closed list of diseases), and treatment (number and type of drug prescribed)—were collected using questionnaires completed by patients included in the study. The number of specific drugs prescribed for one of the diseases considered in the study was recorded at the moment of recruitment.
Two questionnaires to measure HRQoL and work productivity were distributed: 36-item Short Form (SF-36), a generic questionnaire to assess HRQoL,23,24 and Work Productivity and Activity Impairment (WPAI) to evaluate the impact of health status on daily activities.25 SF-36 has two components, viz., physical and mental components; both were considered principal variables and were given in median and standard error. WPAI has the following variables: absenteeism, loss of productivity, global loss of productivity, and restriction on daily activities, which has been calculated according to the instructions given by researchers.26 The former constituent variables of SF-36 and WPAI were compared between the four groups of patients. Each variable was calculated by one-way ANOVA. Adjusted logistic regression was performed using analysis of covariance.
RESULTS
Seventy-four primary care centers were enrolled in the study. A total number of 79 researchers recruited 737 patients. Six hundred sixteen (83,6%) of 737 patients were included in the analysis after considering inclusion and exclusion criteria. One hundred twenty-one patients did not fulfill inclusion criteria or did not give informed consent; thus, they were not considered in the final analysis.
Table 1 summarizes demographic characteristics, comorbidities, and treatment. Statistically significant differences were found for the aforementioned clinical and demographic variables between the four diseases, so a stratified analysis of SF-36 and WPAI scores by sex, physical activity, presence or absence of comorbidity, and number of treatments was performed. There were significant differences in sex distribution, both in AR and depression. Patients suffering from AR were younger and more active, compared with the other three groups. Furthermore, these patients mainly develop intellectually related activities compared with those suffering from the three other pathologies. Taking into account the severity of the patients established by the physician, the percentage of severe patients was significantly higher among the depression group. Table 2 shows scores of GCI distributed in three categories for each disease. Ninety-five percent of AR patients had mild or moderate disease. According to GCI, >50% of the patients in each group have a moderate disease. Table 3 records the values for TSS5 and visual analog scale for AR patients.
Table 1.
Demographic characteristics, comorbidities, and medication of the patients who were assessed and diagnosed with AR, depression, hypertension, and DM
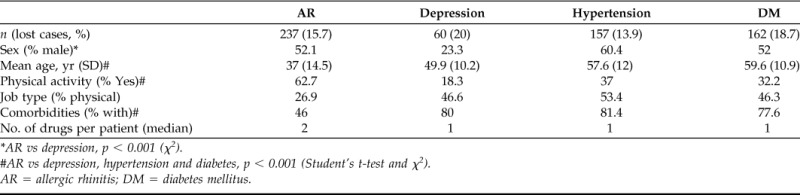
*AR vs depression, p < 0.001 (χ2).
#AR vs depression, hypertension and diabetes, p < 0.001 (Student's t-test and χ2).
AR = allergic rhinitis; DM = diabetes mellitus.
Table 2.
Severity assessment of the AR patients by CGI scale
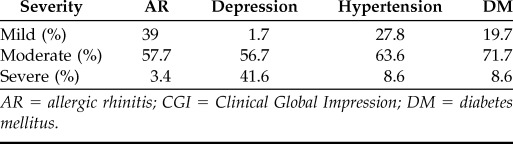
AR = allergic rhinitis; CGI = Clinical Global Impression; DM = diabetes mellitus.
Table 3.
Severity score of AR patients regarding the TSS5
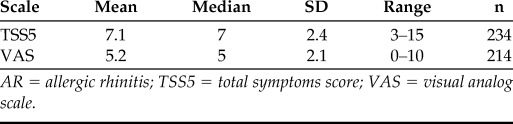
AR = allergic rhinitis; TSS5 = total symptoms score; VAS = visual analog scale.
Quality of Life
SF-36 physical domain scores were significantly different in DM patients (adjusted mean ± SE, 42.4 ± 0.7) compared with AR (46 ± 0.6) and hypertension (45.5 ± 0.7) patients, but not when the former were compared with the depression group patients (43.9 ± 1.1). Mental domain showed vast differences between depression group (21.1 ± 1.2) and the rest of patients. No differences on mental domain scores were found between AR (51.5 ± 0.6), DM (50.6 ± 0.7), and hypertension (50.4 ± 0.7; Fig. 1 and Table 4).
Figure 1.

Assessment of 36-item Short Form (SF-36) physical and mental scales adjusted by age and sex in all four diseases.
Table 4.
SF-36 domains results in all four diseases
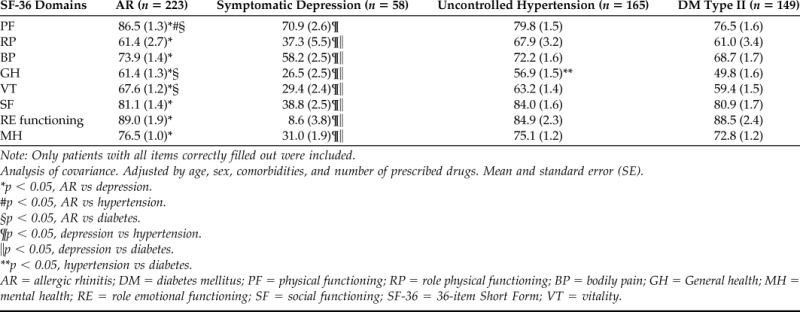
Note: Only patients with all items correctly filled out were included.
Analysis of covariance. Adjusted by age, sex, comorbidities, and number of prescribed drugs. Mean and standard error (SE).
*p < 0.05, AR vs depression.
#p < 0.05, AR vs hypertension.
§p < 0.05, AR vs diabetes.
¶p < 0.05, depression vs hypertension.
=p < 0.05, depression vs diabetes.
**p < 0.05, hypertension vs diabetes.
AR = allergic rhinitis; DM = diabetes mellitus; PF = physical functioning; RP = role physical functioning; BP = bodily pain; GH = General health; MH = mental health; RE = role emotional functioning; SF = social functioning; SF-36 = 36-item Short Form; VT = vitality.
Work Productivity
A total number of 297 patients were in paid employment. Distribution of working status was significantly different comparing AR (60%) with the other groups: depression (37%), hypertension (43%), and DM (35.5%). These differences disappeared after stratifying by age and sex.
Regarding the WPAI analysis, only the 297 employed patients were included in questions related to work. All of the patients were included in terms of day-to-day activities analysis.
Absenteeism and loss of productivity due to illness are summarized in Fig. 2. Absenteeism was higher in the depression group (adjusted mean ± SE, 31.7 ± 2.6%) than among AR (4.6 ± 1.1%), DM (4.2 ± 1.7%) or hypertension patients (2.1 ± 1.5%) featuring statistically significant differences. The other three groups showed no significant differences. Global loss of productivity was significantly higher in the depression group (adjusted mean ± SE, 59.5 ± 4.3%) than in AR (26.6 ± 1.8%), hypertension (8.8 ± 2.5%), and DM (16.7 ± 2.8%). This difference is likewise significant when AR is compared with hypertension and DM groups. With regard to impairment on activities of daily living, depression (adjusted mean ± SE, 59.4 ± 2.6%) and AR (27.8 ± 1.3%) displayed higher scores, eliciting significant differences between depression and the three other groups, as well as between AR and hypertension (19.8 ± 1.6%) but not between AR and DM (25.7 ± 1.6%; Table 5).
Figure 2.

Relationship of the different variables assessed in the questionnaires in allergic rhinitis (AR), depression, hypertension, and diabetes mellitus (DM).
Table 5.
WPAI questionnaires results in AR, depression, hypertension, and DM
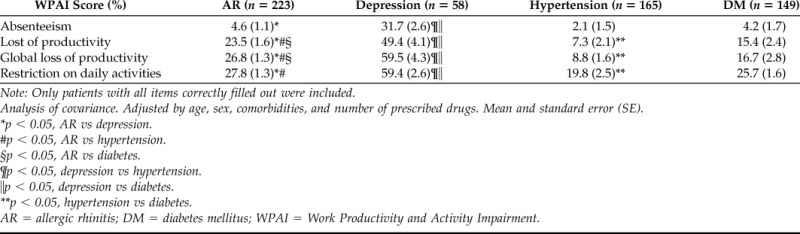
Note: Only patients with all items correctly filled out were included.
Analysis of covariance. Adjusted by age, sex, comorbidities, and number of prescribed drugs. Mean and standard error (SE).
*p < 0.05, AR vs depression.
#p < 0.05, AR vs hypertension.
§p < 0.05, AR vs diabetes.
¶p < 0.05, depression vs hypertension.
=p < 0.05, depression vs diabetes.
**p < 0.05, hypertension vs diabetes.
AR = allergic rhinitis; DM = diabetes mellitus; WPAI = Work Productivity and Activity Impairment.
A moderate correlation was obtained between global loss of productivity and clinical severity, measured by the CGI score, in AR and depression (Table 6). Severe AR patients (TSS5 > 7) have more impact on loss of productivity (30.1 ± 2.6%) and daily activities (33.6 ± 2.1%) than AR total sample, but comparing severe AR with the three other diseases, the results were not as different from those obtained from the whole or total AR sample of patients. Somnolence was acknowledged by 17.8% of AR patients, but correlation between somnolence and productivity loss was not found.
Table 6.
Correlation between CGI scale and global loss of productivity
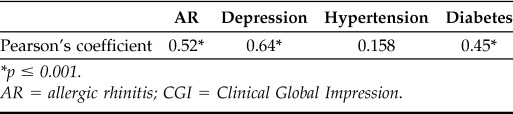
*p ≤ 0.001.
AR = allergic rhinitis; CGI = Clinical Global Impression.
DISCUSSION
Today, it is widely accepted that the great majority of diseases and their respective treatments may affect cognitive or psychomotor functions and subsequently impact work activity. Allergic asthma and rhinitis occur among these diseases. Decreased productivity is evidenced in patients who suffer from moderate or severe rhinitis because of their disease, as established by studies that include large series of patients.15 Moreover, specific rhinitis symptoms, disturbances on sleeping, and the prescription of sedative antihistamines show the highest influence on work productivity.8 In the current study, somnolence was assessed but not as a drug-specific adverse effect. Moreover, it could not be related with loss of productivity. However, AR is seldom compared with other chronic diseases in terms of work functioning, and prospective studies are lacking.
The aim of this study was to evaluate the impact of AR on work activity, in terms of loss of productivity due to illness, compared with other prevalent diseases in the primary care practice. Results obtained support this hypothesis, eliciting 4.1% of absenteeism and 23.5% of presenteeism due to AR, which are higher than other prevalent pathologies, such as DM and hypertension.
In this study, the patients suffering from depression showed the lowest scores in HRQoL and had higher impact on labor activity compared with the three other diseases, consistent with previous reports.27 A recent study in the United States has revealed a high work absenteeism and presenteeism among patients with depression, leading to a great socioeconomic impact on society. It showed a relationship between the severity of depression symptoms and work function and suggests that even minor levels of depression are associated with a loss of productivity.28 For all of these reasons it is not surprising that the impact of depression on work productivity is markedly higher than in the three other diseases studied.
The concurrence of mental disorders with chronic physical disorders is pivotal, because strong mental–physical comorbidities have been found both in general population samples and in primary care samples.29 Common diseases such as asthma, hypertension, or arthritis have an odds ratio of 1.8–2.5 of suffering major depression, as stated previously.12 However, in our study, depressive patients were excluded in the three other groups of diseases evaluated. Therefore, depression could not have influenced the results in AR, hypertension, or diabetes patients.
Hypertension has high mortality and morbidity rates, particularly if organic malfunction occurs. It is accepted that well-controlled hypertension is asymptomatic, but it has been documented as having an impact on QoL because of change of mood, cognitive modifications, or clinical symptoms such as headache or dizziness as well as the use of specific medication.30,31 Nevertheless, several studies underline that symptoms themselves have high impact on QoL, superior to other aspects of the disease, such as type of hypertension or prescribed treatment.32 Some previous articles on work productivity have been published reporting similar results to ours.12 In the present study, the influence of hypertension on this aspect of work is significantly lower than that observed in rhinitis.
DM has an enormous cost both for the individual and for the health system.31 In the United States, DM is among the most expensive of diseases and it is considered to generate one of the highest direct costs for the health system and indirect costs in terms of sick leave or disability.33,34 This last point is not found in other reports where absenteeism due to DM is not very high.35 In our study, the absenteeism percentage is similar to that observed in rhinitis or in hypertension. This can be partly explained by the mean age of the sample (60 years) and by the “healthy-worker” effect. Patients included in this project are closely followed by their physicians and this could explain a lower impact of the disease.
AR has an unquestionable impact on work, measured by WPAI questionnaire.15,36 Moreover, an allergy-specific version of WPAI questionnaire has been developed to assess whether improvement has been fulfilled after treatment.37 In our study we were interested in comparing AR with other chronic diseases and for that purpose a generic version of WPAI, valid for all of them, was distributed. Studies comparing work functioning in AR with other diseases in usual clinical practice conditions are lacking. Results of loss of productivity obtained through clinical trials may not reflect a real situation because a great deal of patients are excluded from these studies.38 Agreeing with us, a recent study in primary care patients (similar to our sample) found an important impairment on work functioning in AR patients in usual clinical practice conditions.39
A previous study comparing work functioning in several common diseases from the employer's perspective8 found a productivity loss in AR of ∼28%, very similar to our results, as is for DM and hypertension patients, but not for depression patients. It showed that AR patients were absent 3.6 days/year because of the former condition and were unproductive 2.3 hours per workday when experiencing symptoms. It concluded that allergies are major contributors to the total cost of health-related absenteeism and presenteeism. Limitations of this study were the lack of evaluation of the severity of the diseases and that, probably, a recall bias could have been present because a 12-month period was inquired.
It is also important to mention that the untoward use of sedative antihistamines in primary care and self-medication have been related to industrial accidents yielding an estimated loss of productivity of 13% in patients taking sedative medication. Patients included in this study have mainly moderate AR and >80% of them were taking symptomatic medication. Approximately 19% of them admitted to suffering from somnolence, but correlation with productivity loss was not found. Previous articles observed that somnolence could affect work functioning,8 but in our study somnolence was evaluated as an open question; hence, it may reduce the accuracy of the results. Numerous patients manage their AR with over-the-counter medications including sedating antihistamines, which could promote somnolence,40 unlike nonsedating H1-blockers.37
Regarding HRQoL, a generic questionnaire was chosen because the comparison between distinct diseases was not feasible by electing a specific one. A specific questionnaire improves the sensitivity and may achieve better correlations with work functioning. High impact of AR on HRQoL and on work productivity could be unexpected for many clinicians, but in previous studies, when AR has been compared with other allergic diseases such as asthma, scores obtained in mental domain are similar.41 Results obtained here follow this trend.
As it has been communicated in previous studies, the severity of the disease—assessed using the CGI scale—correlates with work productivity impairment in depression,28 AR,7 and DM,35 but not in hypertension12 patients. In our study, we observed trends suggestive of work impairment in patients with severe AR but statistical significance was not reached.
Sixteen percent of the total number of patients were considered recruitment failures, because all of the disease groups dropped out in this recruitment period of the study; therefore, it is scarcely probable that this fact affects the final results.
In conclusion, AR induces greater deterioration in work functioning than DM and hypertension. Depression has a higher impact on HRQoL and work productivity than the other diseases.
ACKNOWLEDGMENTS
The authors acknowledge substantial contributions to conception and design of the study and analysis and interpretation of data. They all participated in revising it critically for important intellectual content and final approval of the version to be published.
Footnotes
Funded by Fundación Aragonesa para la Investigación en Alergología (FADIA) and Laboratorios Recordati, Spain
B de la Hoz Caballer, M Rodríguez, J Fraj, I Cerecedo, D Antolín-Amérigo, and C Colás has received grant and research support from Laboratorios Recordati
REFERENCES
- 1. Canonica GW, Bousquet J, Mullol J, et al. A survey of the burden of allergic rhinitis in Europe. Allergy 62(suppl 85):17–25, 2007. [DOI] [PubMed] [Google Scholar]
- 2. Bauchau V, Durham SR. Prevalence and rate of diagnosis of allergic rhinitis in Europe. Eur Respir J 24:758–764, 2004. [DOI] [PubMed] [Google Scholar]
- 3. Gupta R, Sheikh A, Strachan DP, et al. Burden of allergic disease in the UK: Secondary analyses of national databases. Clin Exp Allergy 34:520–526, 2004. [DOI] [PubMed] [Google Scholar]
- 4. Anandan C, Gupta R, Simpson CR, et al. Epidemiology and disease burden from allergic disease in Scotland: analyses of national databases. J R Soc Med 102:431–442, 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bousquet J, Bullinger M, Fayol C, et al. Assessment of quality of life in patients with perennial allergic rhinitis with the French version of the SF-36 Health Status Questionnaire. J Allergy Clin Immunol 94:182–188, 1994. [DOI] [PubMed] [Google Scholar]
- 6. Blanc PD, Trupin L, Eisner M, et al. The work impact of asthma and rhinitis: Findings from a population-based survey. J Clin Epidemiol 54:610–618, 2001. [DOI] [PubMed] [Google Scholar]
- 7. Benninger MS, Benninger RM. The impact of allergic rhinitis on sexual activity, sleep, and fatigue. Allergy Asthma Proc 30:358–365, 2009. [DOI] [PubMed] [Google Scholar]
- 8. Lamb CE, Ratner PH, Johnson CE, et al. Economic impact of workplace productivity losses due to allergic rhinitis compared with select medical conditions in the United States from an employer perspective. Curr Med Res Opin 22:1203–1210, 2006. [DOI] [PubMed] [Google Scholar]
- 9. Hellgren J, Cervin A, Nordling S, et al. Allergic rhinitis and the common cold—High cost to society. Allergy 65:776–783, 2010. [DOI] [PubMed] [Google Scholar]
- 10. Crystal-Peters J, Crown WH, Goetzel RZ, et al. The cost of productivity losses associated with allergic rhinitis. Am J Manag Care 6:373–378, 2000. [PubMed] [Google Scholar]
- 11. Blaiss MS. Allergic rhinitis: Direct and indirect costs. Allergy Asthma Proc 31:375–380, 2010. [DOI] [PubMed] [Google Scholar]
- 12. Kessler RC, Ormel J, Demler O, et al. Comorbid mental disorders account for the role impairment of commonly occurring chronic physical disorders: Results from the National Comorbidity Survey. J Occup Environ Med 45:1257–1266, 2003. [DOI] [PubMed] [Google Scholar]
- 13. Valovirta E, Myrseth SE, Palkonen S. The voice of the patients: Allergic rhinitis is not a trivial disease. Curr Opin Allergy Clin Immunol 8:1–9, 2008. [DOI] [PubMed] [Google Scholar]
- 14. Simoens S, Laekeman G. Pharmacotherapy of allergic rhinitis: A pharmaco-economic approach. Allergy 64:85–95, 2009. [DOI] [PubMed] [Google Scholar]
- 15. Bousquet J, Neukirch F, Bousquet PJ, et al. Severity and impairment of allergic rhinitis in patients consulting in primary care. J Allergy Clin Immunol 117:158–162, 2006. [DOI] [PubMed] [Google Scholar]
- 16. Berk M, Ng F, Dodd S, et al. The validity of the CGI severity and improvement scales as measures of clinical effectiveness suitable for routine clinical use. J Eval Clin Pract 14:979–983, 2008. [DOI] [PubMed] [Google Scholar]
- 17. International Rhinitis Management Working Group. International Consensus Report on the diagnosis and management of rhinitis. Allergy 49 (Suppl 19):1–34, 1994. [PubMed] [Google Scholar]
- 18. Juniper EF, Stahl E, Doty RL, et al. Clinical outcomes and adverse effect monitoring in allergic rhinitis. J Allergy Clin Immunol 115:S390–S413, 2005. [DOI] [PubMed] [Google Scholar]
- 19. Bousquet PJ, Combescure C, Neukirch F, et al. Visual analog scales can assess the severity of rhinitis graded according to ARIA guidelines. Allergy 62:367–372, 2007. [DOI] [PubMed] [Google Scholar]
- 20. Guy W. ECDEU Assessment Manual for Psychopharmacology. Bethesda, MD: National Institute of Mental Health, US Dept Health, Education and Welfare publication (ADM) 76–338; pp. 218–222, 1976. [Google Scholar]
- 21. World Health Organization. WHO initiative on depression in public health. www.who.int/mental_health/management/depression/depressioninph/en/
- 22. World Health Organization. Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia. www.whqlibdoc.who.int/publications/2006/9241594934_eng.pdf
- 23. Alonso J, Prieto L, Anto JM. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): an instrument for measuring clinical results. Med Clin (Barc) 104:771–776, 1995. [PubMed] [Google Scholar]
- 24. Alonso J, Regidor E, Barrio G, et al. Population reference values of the Spanish version of the Health Questionnaire SF-36. Med Clin (Barc) 111:410–416, 1998. [PubMed] [Google Scholar]
- 25. Gawlicki MC, Reilly MC, Popielnicki A, et al. Linguistic validation of the US Spanish work productivity and activity impairment questionnaire, general health version. Value Health 9:199–204, 2006. [DOI] [PubMed] [Google Scholar]
- 26. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics 4:353–365, 1993. [DOI] [PubMed] [Google Scholar]
- 27. Lerner D, Adler DA, Chang H, et al. The clinical and occupational correlates of work productivity loss among employed patients with depression. J Occup Environ Med 46:S46–S55, 2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Beck A, Crain AL, Solberg LI, et al. Severity of depression and magnitude of productivity loss. Ann Fam Med 9:305–311, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Berardi D, Berti Ceroni G, Leggieri G, et al. Mental, physical, and functional status in primary care attenders. Int J Psychiatry Med 29:133–148, 1999. [DOI] [PubMed] [Google Scholar]
- 30. Erickson SR, Williams BC, Gruppen LD. Relationship between symptoms and health-related quality of life in patients treated for hypertension. Pharmacotherapy 24:344–350, 2004. [DOI] [PubMed] [Google Scholar]
- 31. Ogunlana MO, Adedokun B, Dairo MD, et al. Profile and predictor of health-related quality of life among hypertensive patients in south-western Nigeria. BMC Cardiovasc Disord 9:25, 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Erickson SR, Williams BC, Gruppen LD. Perceived symptoms and health-related quality of life reported by uncomplicated hypertensive patients compared to normal controls. J Hum Hypertens 15:539–548, 2001. [DOI] [PubMed] [Google Scholar]
- 33. American Diabetes Association. Economic costs of diabetes in the U.S. In 2007. Diabetes Care 31:596–615, 2008. [DOI] [PubMed] [Google Scholar]
- 34. Ramsey S, Summers KH, Leong SA, et al. Productivity and medical costs of diabetes in a large employer population. Diabetes Care 25:23–29, 2002. [DOI] [PubMed] [Google Scholar]
- 35. Lavigne JE, Phelps CE, Mushlin A, et al. Reductions in individual work productivity associated with type 2 diabetes mellitus. Pharmacoeconomics 21:1123–1134, 2003. [DOI] [PubMed] [Google Scholar]
- 36. Bousquet J, Demarteau N, Mullol J, et al. Costs associated with persistent allergic rhinitis are reduced by levocetirizine. Allergy 60:788–794, 2005. [DOI] [PubMed] [Google Scholar]
- 37. Okubo K, Gotoh M, Shimada K, et al. Fexofenadine improves the quality of life and work productivity in Japanese patients with seasonal allergic rhinitis during the peak cedar pollinosis season. Int Arch Allergy Immunol 136:148–154, 2005. [DOI] [PubMed] [Google Scholar]
- 38. Costa DJ, Amouyal M, Lambert P, et al. How representative are clinical study patients with allergic rhinitis in primary care? J Allergy Clin Immunol 127:920–926 e921. [DOI] [PubMed] [Google Scholar]
- 39. Szeinbach SL, Seoane-Vazquez EC, Beyer A, et al. The impact of allergic rhinitis on work productivity. Prim Care Respir J 16:98–105, 2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Fireman P. Treatment of allergic rhinitis: Effect on occupation productivity and work force costs. Allergy Asthma Proc 18:63–67, 1997. [DOI] [PubMed] [Google Scholar]
- 41. Leynaert B, Neukirch C, Liard R, et al. Quality of life in allergic rhinitis and asthma. A population-based study of young adults. Am J Respir Crit Care Med 162:1391–1396, 2000. [DOI] [PubMed] [Google Scholar]