
Figure 2.
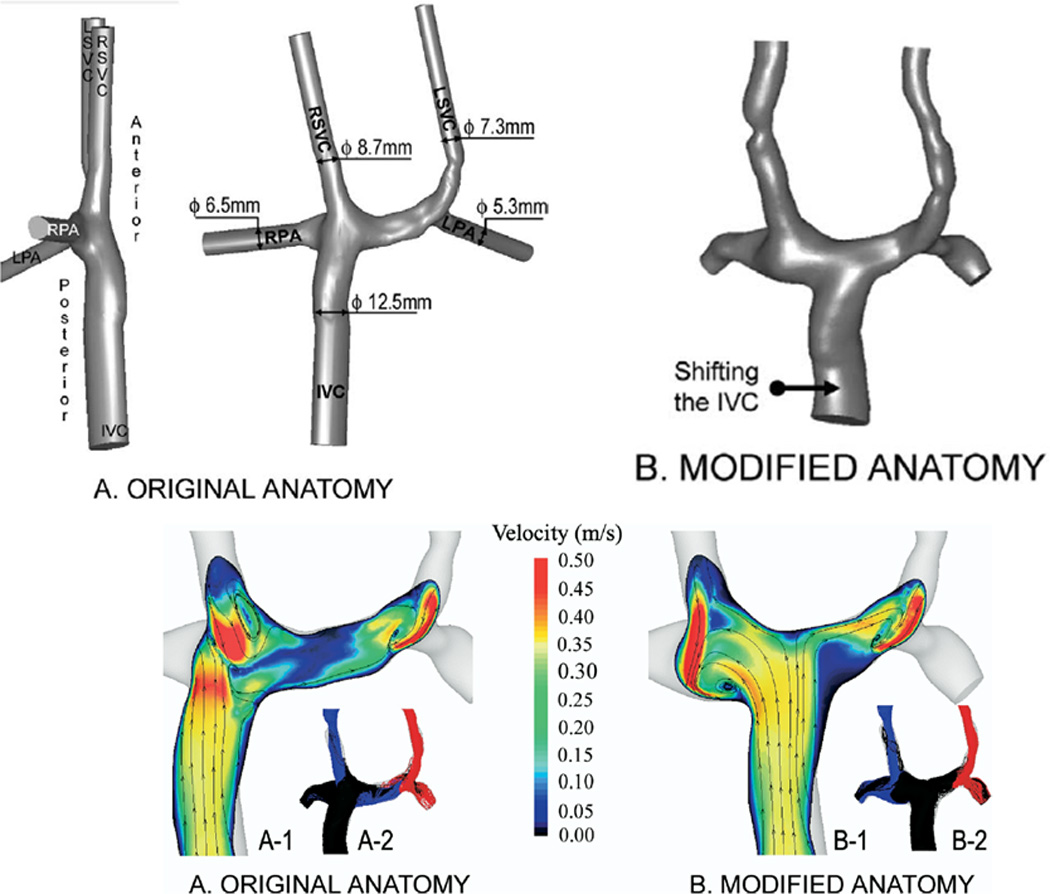
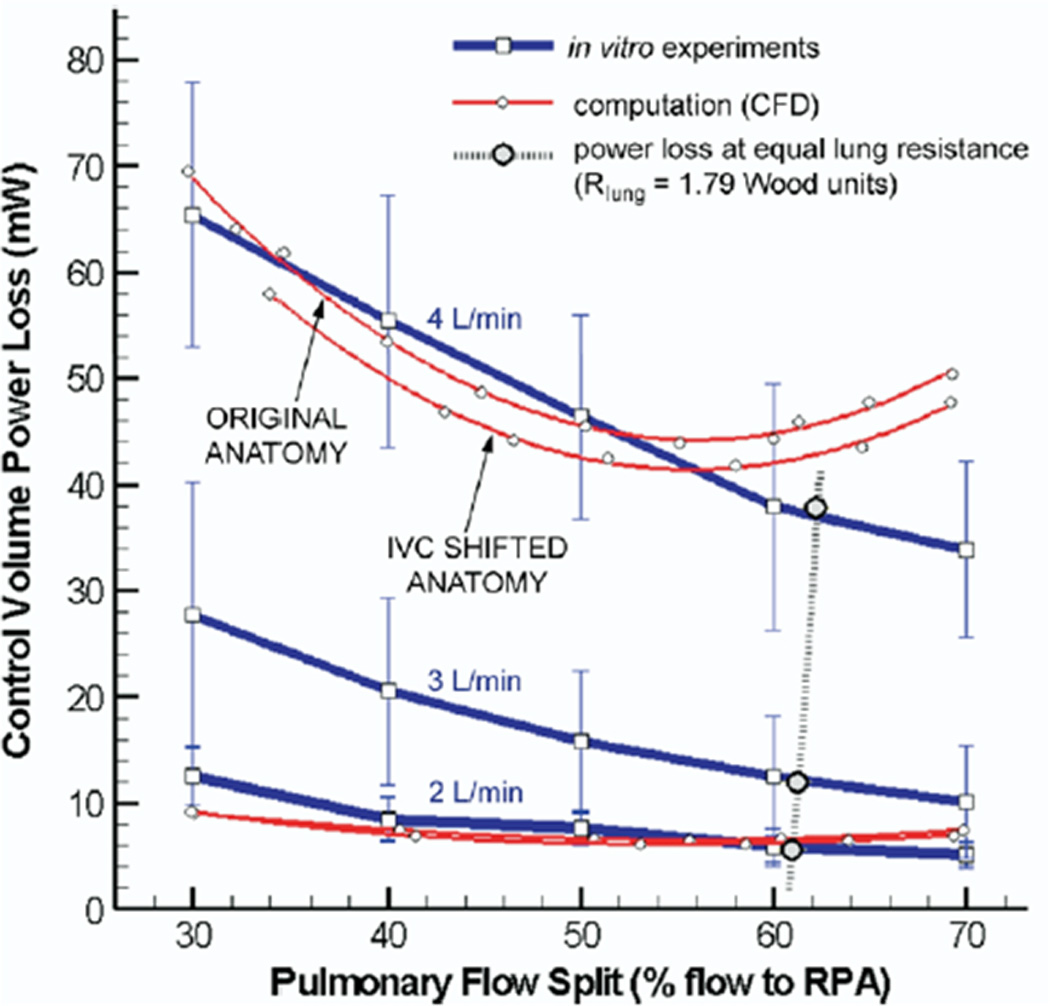
Surgical planning utilized in a bilateral bidirectional Glenn/Fontan patient. (A). (Top) Original anatomy of the Fontan baffle and bilateral bidirectional Glenn connection is on the left; note the Fontan baffle is directly below the right superior vena cava (RSVC). On the right, the baffle is moved by “virtual surgery.” (Bottom) Velocities as calculated by CFD in the original anatomy (left) and by virtual surgery (right). Note the low velocities in the central pulmonary artery in the original anatomy. (B). Graph of power loss on the Y axis and percent flow to the right pulmonary artery (RPA) on the X axis for the original anatomy and the virtual surgery (inferior vena cava, IVC shifted anatomy) for in-vitro flow experiments (blue line) and CFD (red lines) at 3 different flow rates. Note at 4 l/min where the comparison was performed, the virtual surgery anatomy performs better than the original anatomy with lower PL. Note that the in-vitro measurements and CFD differ at that flow because of instabilities (Reynold’s number > 2299 in the RPA at 70:30 RPA/LPA), reaching the limitations of the commercial CFD package used. LSVC=superior vena cava, LPA=left pulmonary artery, m/s=meters per second. From de Zélicourt D, Pekkan K, Parks J, Kanter K, Fogel M, Yoganathan AP. Flow Study of an Extra-Cardiac Connection with Persistent Left Superior Vena Cava. J Thorac Cardiovasc Surg. 2006;131:75–791. With permission.