

Abstract
Aims
To accurately document the amount of quitting, length of quit attempts, and prevalence of plans and serious thought about quitting among smokers.
Design
We used longitudinal data from 7 waves of the International Tobacco Control Policy Evaluation 4-Country Survey (ITC-4). We considered point-prevalence data and cumulative prevalence over the 7 years of the study. We also derived annual estimates of quit activity from reports of quit attempts starting only within more recent timeframes, to control for biased recall.
Setting
Australia, Canada, the United Kingdom, and the United States of America.
Participants
21 613 smokers recruited across 7 waves.
Measurements
Reported lifetime quit attempts, annual quit attempts, length of attempts, time since last attempt started, frequency of aborted attempts, plans to quit, and serious thought about quitting.
Findings
Around 40.1% (95% CI: 39.6-40.6) of smokers report attempts to quit in a given year and report an average of 2.1 attempts. Based on free recall, this translates to an average annual quit attempt rate of 0.82 attempts per smoker. Estimates derived only from the preceding month to adjust for recall bias indicate an annual rate of around 1 attempt per smoker. There is a high prevalence of quit-related activity, with over a third of smokers reporting thoughts or actions related to quitting in a given month. Over half the surveyed smokers eventually succeeded in quitting for at least 1 month, and a majority of these for over 6 months.
Conclusions
Smokers think a lot about stopping and make many unsuccessful quit attempts. Many have been able to last for extended periods and yet they still relapsed. More attention needs to be focussed on translating quit-related activity into long-term abstinence.
Keywords: Smoking cessation, rates of quitting, memory effects, sociodemographic effects
Introduction
Quitting smoking successfully is difficult, but there has been little attention given to the amount of unsuccessful quitting activity. Different strategies exist for measuring quit attempts, each with their own limitations. Consequently, current estimates of the amount of quitting activity vary considerably. We try to standardize this, where possible, by converting estimates to average annual quit attempt rates per smoker.
Past studies have found that ex-smokers recalled an average of around 4.7 lifetime quit attempts, whereas current smokers recalled 5 to 6, with 81% recalling at least one attempt of any duration [1,2]. For an average smoking career of 20 years, this would suggest only 25-30% making attempts in any one year, but most estimates of yearly quitting activity are higher than this, ranging from 38.7% to 46.1% [3-6], which suggests a non-trivial rate of forgetting. Quit attempt definitions vary as to whether attempts of less than 24 hours are considered [1,3,5] or not [4], with the latter excluding a substantial proportion of attempts, possibly from more dependent smokers [7]. Furthermore, there is no consistency in the way that multiple attempts made in the same year are incorporated into yearly estimates.
We took data from the UK Smoking Toolkit Study [3] (where smokers recalling more than 3 attempts were excluded) and computed that the remaining smokers made 0.52 quit attempts per smoker per yeara. This value was not adjusted for forgetting, which the authors estimated could be up to 92% for short attempts made months or more earlier. Thus the actual rates of quitting are higher. Others have also found that reported attempts decline with time [8], so estimates of forgetting need to be included in estimates of quitting activity.
Gilpin and Pierce [4] estimated that relapse rates after 30 days are about 18% higher when calculated from the most recent 4 months compared with 9 to 12 months ago, i.e., differential forgetting. West [6] estimated 7-day relapse rates to be around 22% higher when calculated from 1 to 4 weeks ago compared with 4 to 8 weeks ago, and shorter attempts were especially likely to be forgotten, with 80% of attempts lasting under 24 hours forgotten after just one week. Using estimates based only on the preceding month, West concluded that smokers make on average around 1.5 to 1.7 quit attempts per year. Longer attempts are forgotten too, with estimates suggesting 63% of attempts lasting 1 to 7 days forgotten after 6 months, as are around 40% of attempts lasting 1 week to 1 month [3]. This, however, may overstate actual activity because it assumes no digit bias from telescoping of more distant attempts into the target periods. Reports on timing of recency of quit attempts show peaks at 1 week, 1 month and other standard points, suggesting some migration of reports to those points from surrounding times. Consequently, the amount of quitting activity may be overestimated when commonly reported time intervals are used as upper bounds for the target periods, and this digit bias effect needs to be controlled for.
Successful quitting is often defined by length of abstinence, with typical criterion lengths ranging between one to six months [9-11]. Yet not much data is available on what proportion of current smokers have reached and passed these thresholds and subsequently relapsed. Among smokers reporting up to 3 “serious” attempts during the past year, 37.5% lasted more than one month on their most recent attempt [3]. Attempts lasting at least six months were reported by 13% of smokers who made a quit attempt exceeding 24 hours in the past year [12]. When relying only on self-reports, around 29% of quit attempts appear to exceed 3 months, but this estimate drops to 8% when iterative methods are used to adjust for rates of forgetting on relapse curves [13]. Evidence suggests that factors that help maintain longer-term abstinence differ from those involved in the short term [14]. Even though the length of a “typical” quit attempt is likely to vary across time and populations, it would be useful to ascertain the likelihood of reaching certain milestones, as relapse rates continue to decline with increasing length of abstinence.
Selective forgetting of certain types of quit attempts can have important consequences for research outcomes. For example, shorter unsuccessful attempts may be recalled more often when extensive assistance, such as nicotine replacement therapy, is used, leading to an underestimation of the effectiveness of such aids [3,6]. In contrast, policy-based interventions such as tax increases on tobacco can appear to be more effective when quit attempts made before and after the intervention are compared retrospectively, because the forgetting of attempts made longer ago is likely contributing to the comparatively lower quit rates observed prior to the intervention [8]. These issues highlight the importance of controlling for biased recall when evaluating retrospective survey data. A key point is that results derived from cross-sectional analyses must be complemented by longitudinal data.
Making attempts is usefully seen as the end point in a process of contemplation and preparation. It is also useful to consider activity that does not result in actually making attempts, but indicates some strong intention to do so. In Western populations, 10-20% of smokers typically report planning to quit in the next month, and as many as 30% report seriously thinking about making an attempt in the next month [2]. Others have found 46% of smokers say they intend to quit within the next year [13]. Since only around 10% report quit attempts each month, many planned attempts clearly never eventuate. To our knowledge, data on “aborted attempts” has not been published.
The present study aims to better document the amount of quitting activity and patterns of forgetting of quit attempts among smokers in Australia, Canada, the UK and USA, using longitudinal data from the International Tobacco Control 4-Country (ITC-4) survey. We also estimate the prevalence of unsuccessful attempts of varying length, with large samples allowing us to estimate bias in reporting. Finally, we compare different measurement approaches for documenting the amount of quit activity and explore the prevalence of plans and aborted attempts to stop smoking.
Methods
Data collection and sample
A stratified random sample of 21 613 smokers from Australia, Canada, the UK, and USA were recruited via random-digit dialling and computer-assisted telephone interviews over seven waves (2002 – 2008) of the ITC-4 study (see Table 1). Approximately 2000 smokers were surveyed per country per wave, retaining those who quit, and with those lost to attrition replenished from the same sampling frame. Response rates for the eligible smokers we contacted ranged between 55-74% across the 7 waves (see [15; http://www.itcproject.org/research]).
Table 1.
Demographics by wave of the ITC 4-country survey sample.
| Wave 1 (2002) | Wave 2 (2003) | Wave 3 (2004) | Wave 4 (2005) | Wave 5 (2006) | Wave 6 (2007) | Wave 7 (2008) | Totala | |
|---|---|---|---|---|---|---|---|---|
| N (new recruits/recontacted)b | 9058 / --- | 1714 / 6764 | 2552 / 5827 | 2126 / 5979 | 2638 / 5605 | 2329 / 5865 | 1196 / 6010 | 21613 |
| Mean inter-wave interval (SD)c | --- | 203 (19) | 389 (32) | 461 (58) | 362 (32) | 337 (39) | 397 (50) | 355 (38) |
| Percentage of males | 45.3 | 45.0 | 44.2 | 42.9 | 42.7 | 43.1 | 45.1 | 45.4 |
| Mean age (SD)d | 41.4 (14.4) | 43.2 (14.3) | 44.7 (14.1) | 46.3 (14.1) | 47.2 (13.9) | 48.4 (13.8) | 50.5 (13.3) | 43.0 (14.5) |
| Percentage by Country: | ||||||||
| Australia | 25.4 | 25.2 | 25.1 | 25.0 | 26.3 | 26.5 | 24.6 | 22.2 |
| Canada | 24.4 | 25.9 | 25.2 | 25.0 | 24.5 | 24.6 | 25.6 | 24.4 |
| United Kingdom | 26.5 | 25.0 | 24.8 | 25.2 | 24.5 | 24.5 | 25.3 | 24.3 |
| United States | 23.6 | 23.9 | 24.9 | 24.7 | 24.7 | 24.4 | 24.5 | 29.1 |
Total values are based on the number of unique individuals across all seven waves of the study.
Recontacted participants were those present in the directly preceding wave (n = 1600 took part in all 7 waves).
Inter-wave intervals represent the time elapsed (in days) between the current and previous survey waves, for recontacted participants.
Age at each wave is estimated on the basis of participants' reported age (in years) at recruitment plus the time elapsed (in days) between their recruitment survey date and the main survey date for that wave. Data on survey date for wave 7 was missing for 9.7% of participants. Mean total age for the whole sample is the mean age at recruitment.
Measures
Quit attempts
a) new recruits were asked, “Have you ever tried to quit smoking?”; “How many times have you ever tried to quit smoking?”; and “How long ago did your most recent quit attempt end?”, b) at each follow-up, we asked if and how many times respondents had tried to quit since last being surveyed. In addition, in wave 7 we asked, “How long ago did your most recent quit attempt start?”
Length of attempts
a) new recruits were asked, “Of all the times you ever tried to quit smoking, what was the longest period you stayed off cigarettes completely?” b) at each follow-up, we asked “What was the longest time you stayed smoke free since last being surveyed?” The length of the most recent failed attempt was also assessed at waves 5, 6, and 7 by asking “How long were you quit for on your most recent attempt?”
Successfully quit
in subsequent waves, quit status was determined by asking if participants were still smoking or currently quit. Those who were still quit at the next follow-up (approximately 12 months later) and confirmed being quit for the entire inter-wave-interval were considered successfully quit.
Plans to quit
we asked, “Are you planning to quit smoking (within the next month, within the next 6 months, sometime in the future beyond 6 months, or not planning to quit)?” For the present analyses, only reported plans to quit within the next month were considered.
Serious thoughts about quitting
we asked, “When was the last time you seriously thought about quitting smoking (within the last month, 1 to 6 months ago, 6 to 12 months ago, 1 to 5 years ago, more than 5 years ago, or never)?”
Aborted attempts
we asked, “Thinking about the last month, were there any occasions when you decided to make a quit attempt, but did not go through with it for some reason?” (only assessed in wave 7).
Quit activity
anyone reporting a quit attempt, plans to quit, serious thoughts about quitting, and/or an aborted attempt within a given period was defined as having quit activity.
Education
classified as low, moderate, or high, with the tertiles roughly comparable across the differing education systems of the four countries (low: high-school or less, moderate: trade school, technical or community college, or some university but no degree, high: completed university).
Annual household income
classified as low: less than $30 000 (less than £30 000 for the UK), moderate: $30 000 - $59 000 (£30 000 - £44 999 for the UK), high: $60 000 or greater (£45 000 or greater for the UK), or undisclosed: 8.3% of participants declined to state their income and were treated as a separate valid group.
Nicotine dependence
the Heaviness of Smoking Index (HSI) [16] was used, which combines the number of cigarettes smoked per day with the average time between waking and smoking the first cigarette, to obtain 7 levels of dependence from 0 (lowest) to 6 (highest).
Analytic methods
To determine the amount of quitting activity, we first counted the number of reported quit attempts. We then used Equation 1 to estimate the average annual quit attempt rate per smoker from only the more recent attempts, which arguably would be recalled more accurately. To control for digit bias (the preference to respond with categories like weeks and months) we explored the pattern of actual responses rather than stratifying timeframes. Ninety-five percent confidence intervals (95% CI) are presented for prevalence estimates.
| (Eq. 1) |
Results
82.0% of smokers reported having made any quit attempts at recruitment (see Table 2). Those with prior attempts were more likely to be older, female, not from the UK, at least moderately educated, and to have intermediate scores on the HSI. The prevalence of prior attempts was marginally higher, χ2(6) = 19.5, p < .005, among participants who remained in the study for longer (83.8% for 7 waves, 82.4% for 5 waves, and 80.9% for only one wave). Over the course of the study, the proportion of smokers making at least one lifetime quit attempt increased steadily (see Figure 1), reaching 93.8% among those who took part in all 7 waves (10.1% who had reported no attempts prior to recruitment).
Table 2.
Percentage (and 95% confidence intervals) of participants reporting quit attempts, broken down by demographics and dependence.
| Total N | Any prior quit attempts at recruitment | Recent (last 12 months) prior quit attempts at recruitment | Total N for those in at least 5 waves | Attempts over a 5-year perioda | |
|---|---|---|---|---|---|
| Overall percentage | 21613 | 82.0 (81.5-82.5) | 43.0 (42.3-43.6) | 3672 | 76.3 (74.9-77.4) |
| Percentage by age strata | |||||
| 18 – 24 | 2536 | 75.7 (74.0-77.3) | 61.4 (59.5-63.3) | 214 | 88.8 (84.6-93.0) |
| 25 – 39 | 6604 | 81.5 (80.6-82.4) | 47.3 (46.1-48.5) | 940 | 81.5 (79.0-84.0) |
| 40 – 54 | 7633 | 84.0 (83.2-84.8) | 37.8 (36.7-38.9) | 1545 | 72.9 (70.7-75.2) |
| 55 or over | 4840 | 82.6 (81.6-83.7) | 35.7 (34.3-37.0) | 973 | 73.9 (71.1-76.7) |
| Percentage by sex | |||||
| Male | 9815 | 81.7 (79.9-81.4) | 42.2 (41.3-43.2) | 1527 | 73.8 (71.6-76.0) |
| Female | 11798 | 83.0 (82.4-83.7) | 43.6 (42.7-44.5) | 2145 | 78.1 (76.3-79.8) |
| Percentage by country | |||||
| Australia | 4806 | 83.0 (81.9-84.0) | 44.7 (43.3-46.1) | 1083 | 78.0 (75.6-80.5) |
| Canada | 5265 | 84.2 (83.2-85.2) | 44.4 (43.1-45.8) | 974 | 77.8 (75.2-80.4) |
| United Kingdom | 5251 | 78.4 (77.3-79.6) | 39.1 (37.8-40.4) | 946 | 73.3 (70.4-76.1) |
| United States | 6291 | 82.2 (81.3-83.2) | 43.7 (42.5-44.9) | 669 | 75.6 (72.4-78.9) |
| Percentage by income | |||||
| Low | 6711 | 81.5 (80.6-82.5) | 44.6 (43.4-45.8) | 1039 | 75.9 (73.3-78.5) |
| Moderate | 7109 | 82.1 (81.3-83.0) | 42.0 (40.9-43.2) | 1308 | 76.1 (73.8-78.5) |
| High | 5990 | 82.7 (81.7-83.7) | 43.1 (41.9-44.4) | 1088 | 77.3 (74.8-79.8) |
| Not disclosed | 1803 | 80.4 (78.6-82.3) | 40.4 (38.1-42.6) | 237 | 74.3 (68.7-79.8) |
| Percentage by education | |||||
| Low | 11697 | 80.8 (80.1-81.6) | 42.9 (42.0-43.8) | 1931 | 74.7 (72.7-76.6) |
| Moderate | 6693 | 84.2 (83.3-85.1) | 43.5 (42.3-44.7) | 1174 | 78.2 (75.8-80.6) |
| High | 3152 | 81.9 (80.5-83.2) | 42.5 (40.8-44.2) | 559 | 77.8 (74.4-81.3) |
| Percentage by dependence (HSI) | |||||
| 0 | 2711 | 77.8 (76.3-79.4) | 47.7 (45.8-49.6) | 448 | 80.6 (76.9-84.2) |
| 1 | 2282 | 81.9 (80.3-83.4) | 48.3 (46.3-50.4) | 367 | 84.2 (80.5-87.9) |
| 2 | 3821 | 82.5 (81.3-83.7) | 45.0 (43.4-46.6) | 621 | 79.1 (75.9-82.3) |
| 3 | 6049 | 83.1 (82.2-84.1) | 41.4 (40.2-42.6) | 1066 | 75.3 (72.7-77.9) |
| 4 | 3769 | 82.9 (81.7-84.1) | 39.4 (37.8-41.0) | 675 | 72.7 (69.4-76.1) |
| 5 | 1905 | 82.2 (80.4-83.9) | 38.5 (36.3-40.7) | 360 | 71.9 (67.3-76.6) |
| 6 | 773 | 80.6 (77.8-83.4) | 36.0 (32.6-39.3) | 107 | 60.7 (51.5-70.0) |
Note: HSI = Heaviness of Smoking Index. Recent prior quit attempts were those occurring within the one-year period prior to completing the first main survey.
The 5-year period included anyone who was followed up for at least 5 years, thus participants from all 7 waves of the survey were considered. Of these, 15.5% were successfully quit, defined as being quit at the 4th and 5th waves surveyed, and for the entire inter-wave-interval.
Figure 1.

Cumulation of quit attempts over time for participants retained for different time periods, from a base of reporting ever having made an attempt at baseline (solid line) or reporting an attempt in the previous year (dashed line). Successful quitters (those currently quit at the time of being surveyed) were included and considered as having made a quit attempt. Error bars represent 95% confidence intervals.
In the year prior to recruitment, 43% of participants reported quit attempts, with these reports declining with increasing age, HSI, and income. Interestingly, the prevalence of recent attempts was lower among those retained for longer (39.2% for 7 waves, 39.0% for 5 waves, and 45.9% for one wave, χ2(6) = 63.6, p < .001). As Figure 1 shows, the percentage of recent attempts cumulates from the baseline of 43%, reaching 76.3% after 5 years and 82.7% making attempts over 7 years. Attempts over the five-year period declined with age (up to age 40) and with HSI beyond a score of 2 (see Table 2). Notably, 15.5% of the sample we retained this long met our criterion of having successfully quit. Success was only clearly related to lower HSI scores, and higher education
During inter-wave intervals 40.1% of smokers reported making quit attempts (see Table 3). When we recoded anyone reporting over 10 attempts as having made 10 (0.7%), the average number of attempts was 2.1% (46.0% reported multiple attempts). Based on the 3 waves with inter-wave intervals closest to one year, this provides an annual quit attempt rate per smoker of 0.82.
Table 3.
Recent quit attempts (since last survey date) at each wave.
| Wave 2 | Wave 3 | Wave 4 | Wave 5 | Wave 6 | Wave 7 | |
|---|---|---|---|---|---|---|
| N Smokers in main wave (% of all people in main wave)a | 6731 (99.5%) | 5613 (96.3%) | 5585 (93.4%) | 5058 (90.3%) | 5204 (88.7%) | 5307 (88.3%) |
| With no recent quit attempts (95% CI) | 63.5% (62.3-64.6) | 57.2% (55.9-58.5) | 57.0% (55.7-58.3) | 59.3% (57.9-60.6) | 60.9% (59.6-62.2) | 61.0% (59.7-62.3) |
| With under 10 reported quit attempts (95% CI) | 32.2% (31.1-33.3) | 39.5% (38.2-40.8) | 39.2% (38.0-40.5) | 37.6% (36.3-39.0) | 37.4% (36.1-38.7) | 37.8% (36.5-39.1) |
| Reporting 10 or more attempts (95% CI) | 0.9% (0.7-1.2) | 1.5% (1.2-1.8) | 1.4% (1.1-1.7) | 1.1% (0.8-1.4) | 1.0% (0.7-1.2) | 0.9% (0.6-1.2) |
| Number of attempts not reported (95% CI) | 3.4% (0.0-0.1) | 1.8% (1.5-2.2) | 2.3% (1.9-2.7) | 2.0% (1.6-2.4) | 0.8% (0.5-1.0) | 0.2% (0.1-0.4) |
| Mean (SD) number of attemptsb | ||||||
| Among smokers who made attempts | 2.00 (1.75) | 2.24 (1.96) | 2.25 (1.93) | 2.12 (1.80) | 2.06 (1.76) | 2.09 (1.73) |
| Among all smokers | 0.73 (1.43) | 0.96 (1.70) | 0.97 (1.69) | 0.86 (1.55) | 0.80 (1.49) | 0.81 (1.49) |
| Number of attempts correlated (r) with the inter-wave intervalb | .047** | .014 | .032* | .006 | .045** | .014 |
Note: All participants in the table took part in at least two consecutive survey waves. Data was missing for 2 participants in wave 2.
All participants in the wave who were smoking at some point during the interval between the previous and current survey date (i.e. excludes those who were quit for the entire inter-wave-interval, and also excludes new recruits at each wave).
This calculation treats those who did not report the number of attempts as having made the average number of quit attempts considering only those who made attempts, and those reporting more than 10 attempts are capped at 10 attempts.
p < .05,
p < .01
At wave 7, we estimated the average annual quit attempt rate per smoker from time intervals of varying recency (e.g. within the last week, within the last 10 days etc, up to one year, see Equation 1 and Figure 2). While there were higher peaks, the average over the first month for attempts lasting at least 24 hours remained fairly stable at a rate of around one attempt per smoker per year, or 1.2 if we include less than daily attempts. Attempts lasting a week or more seemed to be recalled for several months.
Figure 2.
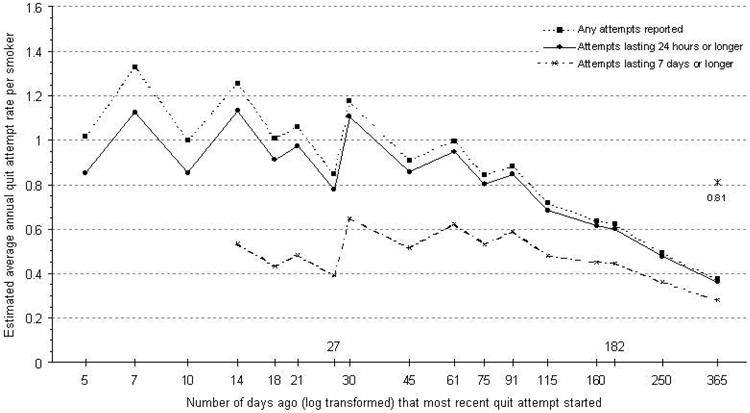
Estimated annual quit attempt rate per smoker for wave 7, based on reported quit attempts starting during different time periods. The reference point at 0.81 is the average reported number of quit attempts based on straight recall for wave 7. Participants quit at the time of the survey but for under 24 hours or under 7 days were excluded from the denominator for the analyses including only attempts lasting at least 24 hours or at least 7 days, respectively. In all analyses, unsuccessful quit attempts spanning the time period of interest (starting before it and ending after it) were excluded. Note that it is not possible to account for multiple attempts by the one individual in these estimates, so accuracy diminishes with longer timeframes.
Table 4 presents the longest ever reported quit attempts made prior to recruitment, then cumulated for subsequent waves. At baseline (see column 1), 54.9% of respondents reported their longest quit attempt lasted a month or more (26.8% 1 – 6 months, and 28.1% longer than 6 months). Among those who reported attempts, only 14.6% were unable to last a week or unable to tell us how long. Over a 5-year period, 68.7% of those starting as smokers had reported quit attempts of at least a month, including 15.5% who met our criteria for being successfully quit. The average length of the most recent quit attempt for wave 7 is displayed in Table 5 (results for waves 5 and 6 were comparable). When we considered relapsed smokers together with those currently still quit (N = 1987), the most recent attempt was reported to last between 1 to 6 days by 21.5%, 7 to 29 days by 29.0% and 30 days or more by 46.2%.
Table 4.
Reported length of longest quit attempts at baseline (ever made prior to recruitment) and after five survey waves (95% confidence intervals are provided in brackets).
| Baseline for all participants | Baseline for those in only one wave | Baseline for those in at least five wavesa | At 5th wave for those in at least five wavesa | |
|---|---|---|---|---|
| N | 21613 | 7516 | 3672 | 3672 |
| No prior attempts | 17.9% (17.4-18.4) | 19.0% (18.1-19.9) | 16.0% (14.9-17.2) | 9.7% (8.7-10.6) |
| < 24 hours | 1.8% (1.6-1.9) | 1.9% (1.6-2.2) | 1.8% (1.3-2.2) | 1.7% (1.3-2.1) |
| 1 – 6 days | 9.5% (9.1-9.9) | 9.8% (9.1-10.4) | 8.8% (7.9-9.7) | 6.9% (6.0-7.7) |
| 7 – 29 days | 15.1% (14.6-15.6) | 15.4% (14.6-16.2) | 14.4% (13.3-15.5) | 13.0% (11.9-14.0) |
| 30 days – 6 months | 26.8% (26.2-27.4) | 27.0% (26.0-28.0) | 26.1% (24.7-27.6) | 26.4% (25.0-27.9) |
| > 6 months | 28.1% (27.5-28.7) | 26.3% (25.3-27.3) | 31.9% (30.4-33.5) | 42.3% (40.7-43.9) |
Note: Data was missing for up to 0.9% of the sample, so columns may not sum to 100%.
The 5-year period included anyone who was followed-up for at least 5 years, thus participants from all 7 waves of the survey were considered. Of these, 15.5% were successfully quit, defined as being quit at the 4th and 5th waves surveyed, and for the entire inter-wave-interval.
Table 5.
Length of most recent quit attempt (relapsed or currently quit) for recontacted respondents in wave 7 who reported making an attempt since they were last surveyed (95% confidence intervals are provided in brackets).
| Relapsed | Still quit | Total | |
|---|---|---|---|
| N | 1398 | 589 | 1987 |
| Shorter than 24 hours | 4.4% (3.4-5.5) | 0.5% (0.0-1.1) | 3.3% (2.5-4.1) |
| 1 to 6 days | 29.3% (26.9-31.6) | 3.2% (1.8-4.7) | 21.5% (19.7-23.3) |
| 7 to 29 days | 36.8% (34.3-39.4) | 10.4% (7.9-12.8) | 29.0% (27.0-31.0) |
| Longer than 29 days | 29.5% (27.1-31.9) | 85.9% (83.1-88.7) | 46.2% (44.0-48.8) |
Note: This table reports data only among current smokers who reported a recent attempt, so the proportion making longer attempts is larger than when a broader sample, including those who did not have attempts, is considered. Data was missing for 3.2% of valid participants.
Within the month prior to being surveyed, 43.8% of smokers in wave 7 indicated some sort of quit activity, including 9.4% reporting attempts and 10.1% aborting planned attempts. Over a year, 71.1% reported activity (see Figure 3). Quit attempts in the previous month were 6.1 (95% CI: 4.9-7.5) times more likely among those with aborted quit attempts than those without. Similarly, quit attempts in the previous month and previous year were 5.3 (95% CI: 4.2-6.6) and 4.4 (95% CI: 3.6-5.5) times more likely, respectively, among participants with plans to quit the following month than those without.
Figure 3.
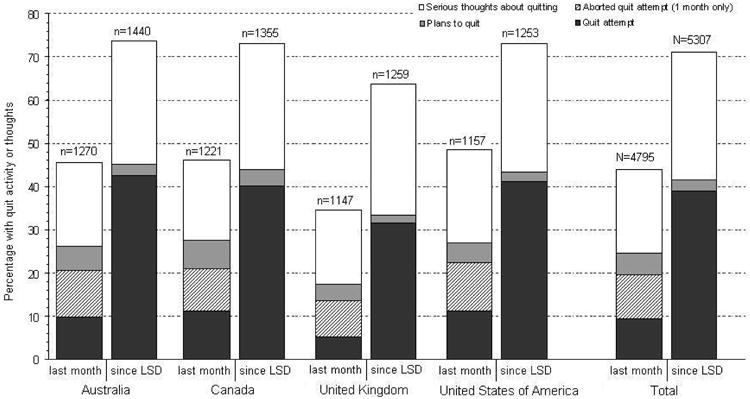
Prevalence of quit related activity within different time periods for smokers in wave 7 (recontacted sample). A quit attempt was defined as a quit attempt starting within the given period of one month (left columns) or since the last survey date, being approximately 12 months (right columns).
There was some cross-country variation in quit activity, with generally lower rates of activity in the UK (see Figure 3). Quit activity decreased with dependence (HSI): over the last year it was 76.8% (95% CI: 73.2-80.5) at the lowest HSI, compared with 62.3% (95% CI: 55.4-69.2) at the highest.
When the index of yearly activity was combined across two waves (around 2 years), 84.4% (95% CI: 83.6-85.3) reported some activity, and when it was extended to three years, 88.6% (95% CI: 87.5-89.8) did so, leaving only 11.4% (95% CI: 10.2-12.5) not reporting any quit-related thoughts or activity over a three-year period.
Discussion
This study illustrates that quit attempts are very common and that thoughts of quitting that do not result in attempts are even more common. Although most quit attempts end rapidly, the majority of smokers have succeeded in staying quit for more than 1 month. In fact, around one third have stopped for more than 6 months.
Our findings suggest less forgetting than some others have found [e.g. 3,6], with only a moderate discrepancy between participants' recall (0.82 attempts per smoker per year) and our estimates based on attempts starting within the past month (around 1 attempt per smoker per year, for attempts lasting at least 1 day), because we controlled for digit bias (see Figure 2). Thus, around 20% of attempts lasting at least one day are forgotten in a year. We suspect that the underreporting of attempts probably results from a combination of forgetting and of some particularly short attempts not being conceptualized as “proper attempts” and so going unreported.
Like attempts made in the past year, lifetime attempts also appear to be underreported. Our data indicates less than 10% of smokers have never tried to quit, despite around 20% reporting never having made a quit attempt at recruitment. Our estimates suggest that the average 40-year-old smoker who started in their teens will have made over 20 failed quit attempts. This speaks clearly to the difficulty of successfully quitting, even when most smokers have at some time abstained for at least a month before relapsing.
It would be useful to determine how prior patterns of quit attempts influence subsequent attempts and the likelihood of quit success. Would smokers be better off trying less often, but putting in more effort and using more help when they do, or does the random element of success call out for a “try and try again” approach? The conditioning associated with past attempts (and failures) and individuals' interpretations of their quitting experiences may combine in ways that are potentially beneficial or harmful for long-term success. Similarly, the relationship between thoughts without actual attempts and later quit outcomes are of interest. It is notable in this regard that those who reported attempts were also much more likely to also report aborted attempts, and, similarly, recent attempts predicted future plans to quit. Smoking cessation is clearly on the minds of most smokers on a fairly regular basis, and we suspect this is important for driving attempts that do eventually happen. It would be informative to systematically explore whether lots of thinking results in more or less attempts over time.
The finding that many failed quit attempts last at least a month, or even 6 months (a common criterion of long-term success in clinical trials) suggests that a key challenge for smoking cessation is helping smokers stay quit longer term. Unfortunately, strategies to reduce longer-term relapse are few [17,18]. The relationship between relapse and some of its key determinants, such as frequency of strong urges to smoke, seems to change at around 1 month [14,19], which suggests that changing strategies somewhere around one month into an attempt may be important, perhaps due to self-regulatory exhaustion [20].
The need for a focus on maintenance should not lead us to ignore the minority who are resistant to quitting at all. Our analysis suggests two groups of smokers without any recent quitting activity: those with no apparent interest (a smallish group) and those who think about it but take no action (a more sizeable group). Among those who have made quit attempts, there are those who have had trouble staying quit for any appreciable length of time, and those who have been able to stay quit through the early difficult period. Each of these four groups might benefit from different interventions.
A limitation of our findings, as with much of the published literature on quit attempts, is that the smokers are from high-income countries with a long history of efforts to educate the population about the risks of smoking. Rates of quitting activity in low- and middle-income countries where information about the health risks of smoking have only recently been publicly disseminated are likely to be much lower [21]. Similarly our findings may not reflect the experiences of very disadvantaged smokers within the four countries studied (e.g. the homeless and those with chronic mental health problems) as they have much higher smoking rates and are underrepresented in surveys of this kind.
The demographic variations we found are of some interest. We observed less quitting activity in the UK, something others [22] have already reported on using much of the same data. However, medium term quit success rates were higher in the UK, so this is not necessarily a negative. Higher education was associated with more quit attempts over the lifespan, whereas lower income was associated with more recent attempts. This may relate to differential memory, or to different motivators for these groups. The more educated might be more aware of smoking-related harms, and thus have quitting on their long-term agenda, whereas the poor might focus more on shorter term needs to quit to save money and thus be less primed to remember the past. The prevalence of recent quit activity was lower among older participants. This group are less interested in quitting, less confident in their ability to quit, perceive fewer health benefits of quitting and hold more self-exempting beliefs about smoking-related harms [12,23]. Finally, consistent with the established literature [24], we found that more dependent smokers made fewer quit attempts and were less likely to succeed.
To conclude, there is a huge amount of unsuccessful quitting activity going on among smokers. Even a small increase in the success rate would have significant effects on prevalence. Whether this would be best achieved by encouraging better use of effective aids or encouraging even more activity is unclear. We need to review what we consider to be success when around one third of current smokers have achieved that milestone (6 months abstinence) in the past. Should we accept this as inevitable and celebrate the benefits of the periods of abstinence or should we be doing more to reduce long-term relapse?
Acknowledgments
The ITC Four-Country Survey is supported by multiple grants including R01 CA 100362 and P50 CA111236 (Roswell Park Transdisciplinary Tobacco Use Research Center) and also in part from grant P01 CA138389 (Roswell Park Cancer Institute, Buffalo, New York), all funded by the National Cancer Institute of the United States, Robert Wood Johnson Foundation (045734), Canadian Institutes of Health Research (57897, 79551), National Health and Medical Research Council of Australia (265903, 450110, APP1005922), Cancer Research UK (C312/A3726), Canadian Tobacco Control Research Initiative (014578); Centre for Behavioural Research and Program Evaluation, National Cancer Institute of Canada/Canadian Cancer Society. We would like to thank members of the Data Management Core at the University of Waterloo for assistance in preparing the data for this analysis.
Footnotes
Declaration of Interest: The authors declare that they have no competing interests
This value of 0.52 was derived by the present authors from data reported in Berg, An, Kirch et al. [3]. Specifically, N = 11772 smokers, of which n = 4550 with at least one quit attempt in the past year, of which n = 2838 reported one, n = 1038 reported 2, and n = 364 reported 3 quit attempts.
Ethics clearance: All waves of the study have received ethical approval from the relevant institutional review board or research ethics committee at The Cancer Council Victoria (Australia), Roswell Park Cancer Institute (USA), University of Waterloo (Canada), and University of Strathclyde (UK).
References
- 1.Javitz HS, Brigham J, Lessov-Schlaggar CN, Krasnow RE, Swan GE. Association of tobacco dependence and quit attempt duration with Rasch-modeled withdrawal sensitivity using retrospective measures. Addiction. 2009;104:1027–1035. doi: 10.1111/j.1360-0443.2009.02540.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kadia A, Edwards J, Fraser-Lee N, Kunyk D, Lightfoot P, et al. [accessed 15/6/2011];Smoking in the Capital Health Region - Report, Population Health Survey 2002. 2004 http://www.capitalhealth.ca/nr/rdonlyres/emopxvk5uqm4zshk5w2kvrmtx5ziehkg2nvrpotzr2wzrza2f6ufmfeq57ue6yxmqlzbpva5ykqvgbllxo3a5rjsycg/summary5-smokcess-ch.pdf. Archived by WebCite® at http://www.webcitation.org/5zSBzkXTD.
- 3.Berg CJ, An LC, Kirch M, Guo H, Thomas JL, et al. Failure to report attempts to quit smoking. Addict Behav. 2010;35:900–904. doi: 10.1016/j.addbeh.2010.06.009. [DOI] [PubMed] [Google Scholar]
- 4.Gilpin E, Pierce JP. Measuring smoking cessation: Problems with recall in the 1990 California Tobacco Survey. Cancer Epidemiol Biomarkers Prev. 1994;3:613–617. [PubMed] [Google Scholar]
- 5.Shiffman S, Brockwell SE, Pillitteri JL, Gitchell JG. Use of smoking-cessation treatments in the United States. Am J Prev Med. 2008;34:102–111. doi: 10.1016/j.amepre.2007.09.033. [DOI] [PubMed] [Google Scholar]
- 6.West R. [accessed 15/6/2011];Feasibility of a national longitudinal study (‘The Smoking Toolkit Stud’) to monitor smoking cessation and attempts at harm reduction in the UK. 2006 Pilot report. www.smokinginengland.info/Ref/stp001.pdf. Archived by WebCite® at http://www.webcitation.org/5zSCERpH2.
- 7.Hughes JR, Callas PW. Definition of a quit attempt: A replication test. 2010;12:1176–1179. doi: 10.1093/ntr/ntq165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Reed MB, Anderson CM, Vaughn JW, Burns DM. The effect of cigarette price increases on smoking cessation in California. Prev Sci. 2008;9:47–54. doi: 10.1007/s11121-008-0081-1. [DOI] [PubMed] [Google Scholar]
- 9.Hughes JR, Keely JP, Niaura RS, Ossip-Klein DJ, Richmond GES. Measures of abstinence in clinical trials: issues and recommendations. Nicotine Tob Res. 2003;5:13–25. [PubMed] [Google Scholar]
- 10.Velicer WF, Prochaska JO. A comparison of four self-report smoking cessation outcome measures. Addict Behav. 2004;29:51–60. doi: 10.1016/s0306-4603(03)00084-4. [DOI] [PubMed] [Google Scholar]
- 11.Sussman S. Effects of sixty six adolescent tobacco use cessation trials and seventeen prospective studies of self-initiated quitting. Tobacco Induced Diseases. 2002;1:35–81. doi: 10.1186/1617-9625-1-1-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Messer K, Trinidad DR, Al-Delaimy WK, Pierce JP. Smoking cessation rates in the United States: A comparison of young adult and older smokers. Am J Public Health. 2008;98:317–322. doi: 10.2105/AJPH.2007.112060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.West R, McEwen A, Bolling K, Owen L. Smoking cessation and smoking patterns in the general population: a 1-year follow-up. Addiction. 2001;96:891–902. doi: 10.1046/j.1360-0443.2001.96689110.x. [DOI] [PubMed] [Google Scholar]
- 14.Herd N, Borland R. The natural history of quitting smoking: findings from the International Tobacco Control (ITC) Four Country Survey. Addiction. 2009;104:2075–2087. doi: 10.1111/j.1360-0443.2009.02731.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Thompson M, Fong GT, Hammond D, Boudreau C, Driezen P, et al. Methods of the International Tobacco Control (ITC) Four Country Survey. Tob Control. 2006;15:iii12–iii18. doi: 10.1136/tc.2005.013870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Heatherton TF, Kozlowski LT, Frecker RC, Rickert W, Robinson J. Measuring the heaviness of smoking: using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Brit J Addict. 1989;84:791–800. doi: 10.1111/j.1360-0443.1989.tb03059.x. [DOI] [PubMed] [Google Scholar]
- 17.Agboola S, McNeill A, Coleman T, Bee JL. A systematic review of the effectiveness of smoking relapse prevention interventions for abstinent smokers. Addiction. 2010;105:1362–1380. doi: 10.1111/j.1360-0443.2010.02996.x. [DOI] [PubMed] [Google Scholar]
- 18.Segan CJ, Borland R. Does extended telephone callback counselling prevent smoking relapse? Health Educ Res. doi: 10.1093/her/cyr009. in press. [DOI] [PubMed] [Google Scholar]
- 19.Herd N, Borland R, Hyland A. Predictors of smoking relapse by duration of abstinence: findings from the International Tobacco Control (ITC) Four Country Survey. Addiction. 2009;104:2088–2099. doi: 10.1111/j.1360-0443.2009.02732.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Muraven M, Baumeister RF. Self-regulation and depletion of limited resources: Does self-control resemble a muscle? Psychol Bull. 2000:247–259. doi: 10.1037/0033-2909.126.2.247. [DOI] [PubMed] [Google Scholar]
- 21.Borland R, Li L, Driezen P, Wilson N, Hammond D, et al. Patterns of interest in and quitting activity internationally: Findings from the ITC family of studies. Manuscript submitted for publication (copy on file with author) [Google Scholar]
- 22.Gibson JE, Murray RL, Borland R, Cummings KM, Fong GT, et al. The impact of the United Kingdom's national smoking cessation strategy on quit attempts and use of cessation services: Findings from the International Tobacco Control Four Country Survey. Nicotine Tob Res. 2010;12:S64–S71. doi: 10.1093/ntr/ntq119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Yong HH, Borland R, Siahpush M. Quitting-related beliefs, intentions, and motivations of older smokers in four countries: findings from the international tobacco control policy evaluation survey. Addict Behav. 2005;30:777–788. doi: 10.1016/j.addbeh.2004.08.023. [DOI] [PubMed] [Google Scholar]
- 24.Hyland A, Borland R, Li Q, Yong HH, McNeill A, et al. Individual-level predictors of cessation behaviours among participants in the International Tobacco Control (ITC) Four Country Survey. Tob Control. 2006;15:iii83–iii94. doi: 10.1136/tc.2005.013516. [DOI] [PMC free article] [PubMed] [Google Scholar]