

Abstract
Purpose
To compare the long-term efficacy and safety of intravitreal triamcinolon with or without rescue laser therapy (intravitreal triamcinolone injection [IVTA] group), bevacizumab with or without rescue laser treatment (intravitreal bevacizumab injection [IVB] group), or a combination of both with or without rescue laser therapy (IVTA + IVB group), with standard care for patients with macular edema secondary to branch retinal vein occlusion (BRVO).
Methods
We reviewed the medical records of 151 patients treated with intravitreal injection with or without rescue laser for treatment of macular edema caused by BRVO, and who were followed up at 1, 3, 6, 12, and 24 months. During the observation period, rescue grid laser or repeated intravitreal injection with initial drug was performed if recurrence of macular edema was confirmed. Visual acuity, change in visual acuity, and intraocular pressure were compared in each phase.
Results
Totals of 16%, 5.6%, and 0% of participants in the three groups showed significant visual loss of more than three lines of the Snellen chart at last follow-up. The IVTA group was the least effective treatment modality, with statistical significance. The development rates of elevated intraocular pressure were similar among the groups.
Conclusions
Although IVTA yielded effects similar to those of standard grid photocoagulation based on the Standard Care vs Corticosteroid for Retinal Vein Occlusion study, IVB or IVTA + IVB with or without rescue laser treatment resulted in improvement in visual acuity at 24 months after the start of treatment and was associated with few serious adverse side effects. Thus, these approaches could be useful for treating macular edema arising secondary to BRVO.
Keywords: Intravitreal injection, Macular edema, Retinal vein occlusion
Branch retinal vein occlusion (BRVO) is the second most common major retinal vascular disease after diabetic retinopathy [1]. Epidemiologic studies found that the prevalence of BRVO ranged from 0.3% [2] to 1.6% [3], and major risk factors for the condition were increasing age, hypertension, and co-existing cardiovascular disease [2-6].
Macular edema is a major cause of visual acuity loss attributable to BRVO [7-9]. The Branch Vein Occlusion Study [7] found that grid photocoagulation was effective for treatment of macular edema. The Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) project showed that grid photocoagulation was the best option for standard care when used to treat macular edema secondary to BRVO [10].
In recent decades, several novel treatments for BRVO have been introduced in major studies such as the BRAVO [11] and GENOVA studies [12]. However, the effects of such treatments remain unclear [1,9,13]. Furthermore, the cited works did not mimic the true clinical situation in that intravitreal bevacizumab injections (IVBs) were consecutively administered over a 3-month period to form a loading dose, the treatment strategy to be adopted after initial treatment failure was not considered, and lastly, no study has compared intravitreal triamcinolone acetate, bevacizumab, and drug combination injections for the treatment of macular edema secondary to BRVO.
In the present study, we reviewed the medical records of patients treated for visual loss caused by macular edema secondary to BRVO 1) to evaluate whether intravitreal triamcinolone acetate, bevacizumab, and a combination of triamcinolone and bevacizumab injections, with or without rescue laser therapy, improved visual acuity compared with standard care of the type administered in the SCORE study, and 2) to determine whether such treatment modalities reduced unfavorable outcomes in patients with macular edema caused by BRVO, compared with those of the SCORE study.
Materials and Methods
All patients were evaluated and treated by three experienced retinal specialists. Diagnosis of BRVO was based on clinical examination, and macular edema was identified by optical coherence tomography (OCT). The possible treatment options for BRVO associated with macular edema were explained to potential study candidates in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. No institutional review board approval was required because of the retrospective study design. The treatment options were suggested included intravitreal triamcinolone acetonide injection, bevacizumab injection, and injection of a combination of triamcinolone acetonide and bevacizumab by doctor's preference. The "off-label" use of bevacizumab and the potential side-effects, particularly the possibility of development of thromboembolic events and uveitis, were extensively discussed with all patients prior to treatment. Any patient with a recent history of myocardial infarction or cerebral vascular accident, and/or uncontrolled hypertension, which were detected by questionnaires, electrocardiogram, and sphygmomanometer, was not offered bevacizumab. Patients were specifically informed about the process of intravitreal injection and the potential risks of endophthalmitis, uveitis, cataract development, ocular hypertension, and retinal detachment.
This consecutive, retrospective, nonrandomized clinical interventional study included patients from January 2000 through December 2009 at HanGil Eye Hospital, Incheon, Korea. A total of 1,028 patients received one of the various interventions mentioned above, but only 151 patients were enrolled in our study after application of the inclusion and exclusion criteria (Table 1). The injection was performed at least 1 month after symptoms appeared. However, when patients were unsure about the initiation of symptoms, injection was performed as soon as the macular edema was detected. The regimens were determined by the treatment trend of macular edema associated with BRVO at that time, surgeon's preference, and the patient's status, such as economics, systemic health status, and ocular status.
Table 1.
Inclusion and exclusion criteria used in the present study
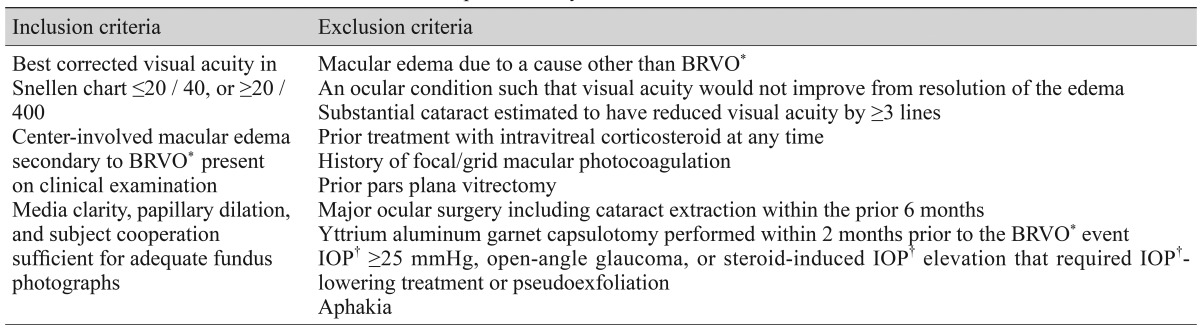
*BRVO = branch retinal vein occlusion; †IOP = intraocular pressure.
Thirty-one patients (31 eyes) were selected without randomization and placed in the intravitreal triamcinolone injection (IVTA) group; each received a single intravitreal injection of 4 mg (0.1 mL) crystalline triamcinolone acetonide (Kenacort-A 40 mg/mL; Bristol-Myers Squibb, Singapore). Another 95 patients (95 eyes), who received a single intravitreal injection of 2.5 mg (0.1 mL) bevacizumab (Avastin 25 mg/mL; Genentech, San Francisco, CA, USA) were placed in the IVB group. The remaining 25 patients (25 eyes), who received a combination of 1.25 mg (0.05 mL) bevacizumab and 2 mg (0.05 mL) triamcinolone acetonide, were placed in the IVTA + IVB group. In the combination group, an additional anterior chamber paracentesis was performed with 20 gauge microincisional blade after the intravitreal injection in order to prevent intraocular pressure increase. During follow-up, rescue grid laser or repeated intravitreal injection with initial drug was performed if recurrence of macular edema was confirmed by fundus examination or OCT.
Each patient underwent a complete ophthalmological examination including standardized visual acuity measurements using Snellen charts, slit-lamp biomicroscopy, Goldmann applanation tonometry, and ophthalmoscopy, at baseline and at 1, 3, 6, 12, and 24 months after treatment. At baseline we performed fluorescein angiography to identify macular ischemia by detecting the enlargement of foveal avascular zone. There were no patients with baseline macular ischemia. Visual acuity, change in visual acuity, and intraocular pressure were compared in each treatment phase. The change in visual acuity was divided into 5 groups associated with the amount of change in visual acuity: visual acuity increased more than 3 lines in Snellen chart, increased 1 to 3 lines, did not change, decreased 1 to 3 lines, or decreased more than 3 lines.
Potential corticosteroid-induced and injection-related complications, if any, were also recorded. No patient had baseline ocular hypertension. Topical anti-glaucomatous medication was prescribed if intraocular pressure was more than 21 mmHg at any follow-up visit. Information on medical history (e.g., hypertension or diabetes) was obtained by chart review. All visual acuity measurements were converted to the logarithm of the minimum angle of resolution scale prior to statistical analysis.
All data are expressed as mean ± standard deviations. The Kruskal-Willis test was used to perform statistical comparisons among the three groups. Analyses were achieved using SPSS ver. 14.1 (SPSS Inc., Chicago, IL, USA). A p-value at 1 month, 3 months, 6 months, 12 months, and 24 months are expressed as p1mon, p3mon, p6mon, p12mon, and p24mon. A p-value less than 0.05 was considered statistically significant.
Results
A total of 151 eyes of 151 patients with BRVO associated with macular edema were included in the present study in which patients were divided into three groups based on intravitreal injection regimen. Mean patient age was 57 ± 10 years in the IVTA group, 58 ± 11 years in the IVB group, and 58 ± 11 years in the IVTA + IVB group, and the proportions of females were 49.2%, 46.9%, and 43.7%, respectively. There were no statistically significant differences among groups in terms of age, gender, preoperative best spectacle-corrected visual acuity, preoperative intraocular pressure, or duration of macular edema (p > 0.05 for all comparisons). No patient dropped out of the study and patient demographics are shown in Table 2.
Table 2.
Baseline characteristics of the treatment groups
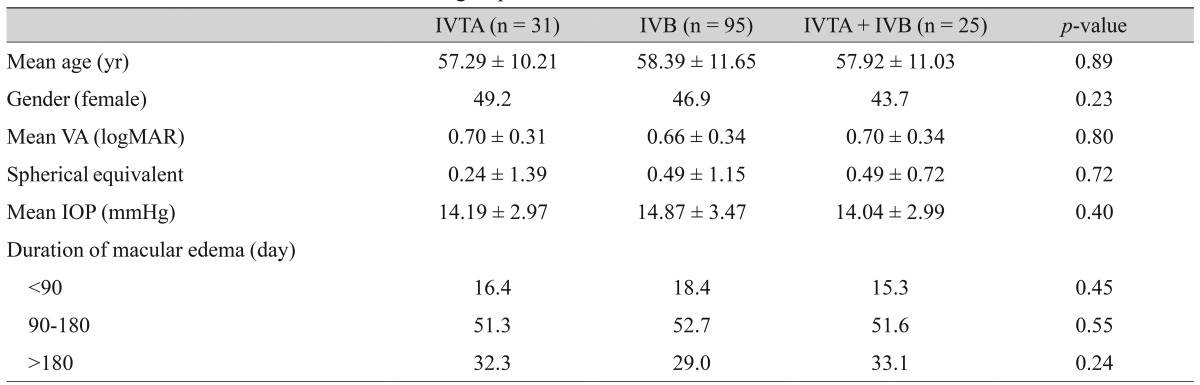
Values are presented as mean ± SD or percent.
IVTA = intravitreal triamcinolone injection; IVB = intravitreal bevacizumab injection; VA = visual acuity; logMAR = logarithm of the minimum angle of resolution; IOP = intraocular pressure.
Visual acuity and intraocular pressure
There were no statistically significant differences in postoperative visual acuity among the three groups at 1, 3, 6, or 24 months postoperatively (p > 0.05). However, at the 12-month follow-up, the IVTA group showed a statistically significant decrease in visual acuity (p = 0.01) (Fig. 1). There was no significant among-group difference in postoperative intraocular pressure at any follow-up time (p1mon = 0.07, p3mon = 0.07, p6mon = 0.63, p12mon = 0.97, and p24mon = 0.23) (Fig. 2).
Fig. 1.

Visual acuity as measured by a Snellen chart at each follow-up interval. The three groups showed no statistically significant difference in visual acuity in most of the follow-up interval except for the 12-month follow-up, at which time the intravitreal triamcinolone injection (IVTA) group showed a statistically significant decrease in visual acuity (graphed on the logarithm of the minimum angle of resolution [logMAR] scale). IVB = intravitreal bevacizumab injection.
Fig. 2.

Intraocular pressure at each follow-up interval. The three groups showed no statistically significant differences in intraocular pressure at any follow-up interval. IVTA = intravitreal triamcinolone injection; IVB = intravitreal bevacizumab injection.
Change in visual acuity
There was no statistically significant difference in change in visual acuity among the three groups at 1, 3, 6, or 24 months postoperatively. However, at the 12-month follow-up, the IVTA group showed less visual improvement than did the other groups, with statistical significance (p = 0.01) (Table 3). The distribution of patients associated with the amount of visual change in each group is schematized in Figs. 3, 4, and 5. Totals of 16%, 5.6%, and 0% of participants in the three groups showed significant visual loss of more than three lines of the Snellen chart at the final follow-up examination.
Table 3.
Post-injection parameters of the treatment groups
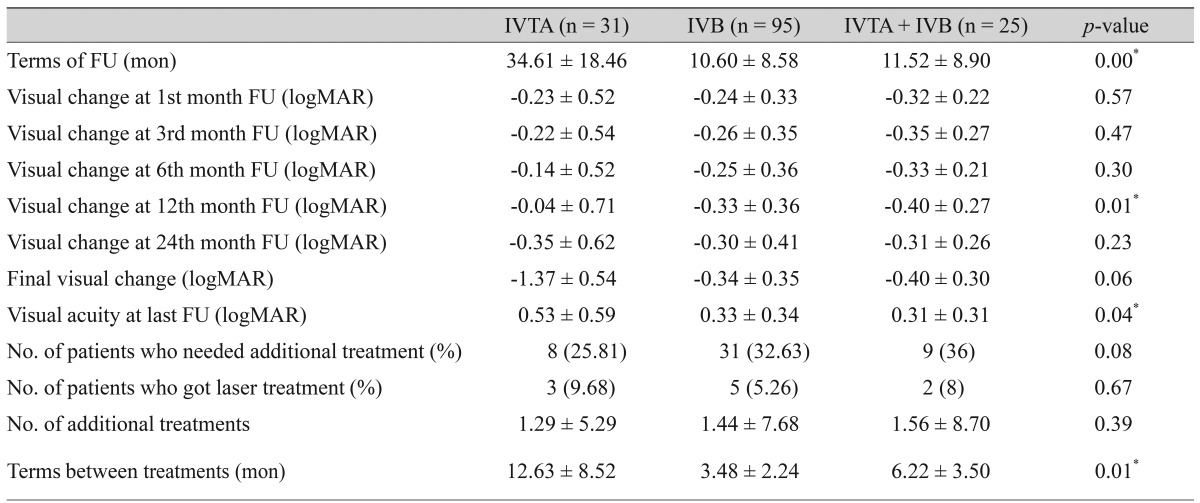
IVTA = intravitreal triamcinolone injection; IVB = intravitreal bevacizumab injection; FU = follow up; logMAR = logarithm of the minimum angle of resolution.
*Statistically significant by Kruskal-Willis test.
Fig. 3.

Patient distribution in the intravitreal triamcinolone injection group with respect to change in visual acuity (VA) differences as measured using a Snellen chart at each follow-up (FU) interval. The levels reflect gain or loss of Snellen chart lines compared with baseline VA.
Fig. 4.

Patient distribution in the intravitreal bevacizumab injection group with respect to change in visual acuity (VA) differences as measured using a Snellen chart at each follow-up (FU) interval. The levels reflect gain or loss of Snellen chart lines compared with baseline VA.
Fig. 5.

Patient distribution in the intravitreal triamcinolone injection + intravitreal bevacizumab injection group with respect to change in visual acuity (VA) differences as measured using a Snellen chart at each follow-up (FU) interval. The levels reflect gain or loss of Snellen chart lines compared with baseline VA.
Length of follow-up and additional treatment
The average length of follow-up for each group is shown in Table 3. IVTA patients were followed-up for longer than the other two groups, with statistical significance. Totals of 25.81% of patients in the IVTA group, 32.63% in the IVB group, and 36% in the IVTA + IVB group required additional treatment during follow-up. The groups did not differ in the frequency of additional treatment or in the number of patients who were referred for laser treatment (p > 0.05), but did vary when the times at which such treatment was needed were compared (p = 0.00) (Table 3).
Discussion
Macular edema is a major cause of visual acuity loss in BRVO patients. Thus, several treatment modalities for macular edema have been developed. One representative strategy is grid laser photocoagulation [10] which is the oldest form of treatment for this condition. As the pathophysiology of macular edema became better understood, several useful drugs were developed. Steroids, including triamcinolone acetonide, and anti-vascular endothelial growth factor (VEGF) antibodies (e.g., bevacizumab) are widely used today.
In many studies, IVTA, IVB, and the combination of both treatments have shown beneficial effects in treatment of macular edema secondary to BRVO. Guthoff et al. [14] compared the intravitreal bevacizumab with triamcinolone acetonide. They concluded that both treatments are effective in reducing central macular thickness, but IVB is more effective in improving visual acuity for 2 months. After 3 months, there is no difference in either group. Ehrlich et al. [15] reported the clinical results of combined treatment using intravitreal bevacizumab and intravitreal triamcinolone in retinal vein occlusion. They concluded that combination treatment showed beneficial effects in improving structural outcomes such as central macular thickness, but had no advantage over results with IVB alone. Cekic et al. [16] compared the three different intravitreal treatment modalities, including intravitreal bevacizumab, intreavitreal triamcinolone, and the combination of both, as in our study. They concluded that all treatment groups had similar therapeutic effects at one month, but at six months, the IVB group had better visual acuity. However, they only analyzed the short term effects of each treatment modality and they did not discuss any visual acuity changes according to treatment used. Of these studies, none were focused on whether a selected treatment might decrease unfavorable outcomes compared with the standard treatment which the SCORE study [10] defined as focal grid photocoagulation.
In the present study, we compared the effects on visual acuity of different treatment regimens in macular edema patients with BRVO. Each treatment tested was similar in effect until 1 year of follow-up. At that time, triamcinolone acetonide was less effective than was bevacizumab or combination therapy when the extent of macular edema was assessed. This conclusion was in line with the finding that additional treatment was needed at approximately 12 months when IVTA was employed. Final visual acuity values were significantly lower in the IVTA group than in the other patients, though this difference may be associated with the fact that the IVTA group had a longer period of follow-up. Thus, a negative selection bias may have been present with respect to IVTA-treated patients.
Patients receiving each of the three treatments required similar numbers of additional injections after the first treatment. Thus, the percentages of patients who received additional treatments, such as another injection or rescue laser therapy, were similar among the three groups. This finding indicates that an initial intravitreal injection did not greatly affect the natural course of disease.
To determine if any chosen treatment decreased unfavorable outcomes, we compared the groups in terms of improvement or deterioration in visual acuity, as was performed in the SCORE study [10]. In the cited work, scoring increments were set by each five letters of the Early Treatment Diabetic Retinopathy Study (ETDRS) chart, equivalent to a single line of difference in a Snellen chart. The data are shown in Figs. 3, 4, and 5. In the SCORE study, 14.9% of patients in the standard care group, 11.6% in the 1 mg IVTA group, and 12% in the 4 mg IVTA group showed decreases in visual acuity of more than three lines of the Snellen chart. In the present study, 16.67% of patients in the IVTA group, 4.76% in the IVB group, and 0% in the IVTA + IVB group showed deterioration in visual acuity of more than three lines at the 12-month follow-up. The results of the IVTA group were similar to those of the SCORE study [10], indicating that additional drug or rescue laser treatment had less effect on visual improvement in this group. In the IVB and IVTA + IVB groups, however, visual loss was much less than that of the standard group in the SCORE study [10], with statistical significance. This difference may reflect a valuable effect of bevacizumab or the fact that rescue laser treatment worked well in both groups. However, as the final visual acuity values at 24 months of follow-up did not differ significantly among the three groups, bevacizumab appeared to maximally influence the other treatment such as triamcinolone acetonide or rescue laser therapy to work well, but not change the natural course of the disease.
The present study had some limitations. First, we did not include a standard care group, but rather obtained such data from the SCORE study [10]. The second limitation is that the number of patients receiving 24-month follow-ups differed among the groups, with more patients available in the IVB group than in the other two groups. This imbalance may have biased our interpretation of the results. Recently, bevacizumab has become a drug of choice for treatment of several retinal diseases and many clinicians choose bevacizumab rather than triamcinolone acetonide because the risks of development of cataracts or glaucoma are lower when the former drug is employed. The third limitation is that OCT data were not compared among groups because, during the follow-up period, OCT techniques evolved rapidly and we switched from use of time domain (TD)-OCT to spectral domain (SD)-OCT. As there is no reliable method to convert TD-OCT data to SD-OCT results, data comparison would be meaningless.
Much effort has been devoted to seeking a cure for macular edema associated with BRVO because the condition is commonly associated with deterioration in visual acuity. One advance in treatment has been the development of anti-VEGF agents, which increase vascular permeability and promote absorption of edema. We compared the effects of triamcinolone acetonide, bevacizumab, and a combination of the two drugs, injected into the vitreous cavity, with or without additional drug treatment or rescue laser therapy, in macular edema patients with BRVO. Although IVTA yielded outcomes similar to those of standard grid photocoagulation in the SCORE study, intravitreal bevacizumab only, or a drug combination with or without rescue laser therapy, resulted in significantly lower visual loss in the present work. Therefore, these two treatment modalities could be used as a substitute for grid laser photocoagulation. However, further clinical studies are warranted to compare the benefits of and tolerance to drug mixing, and application of laser therapy, as well as to gauge the effectiveness of treatment with respect to the size of the foveal avascular zone. Future work with a larger study population and longer follow-up is needed to achieve definite results.
Footnotes
This article was presented as free paper on 11th EURETINA Congress at London in May 2011.
No potential conflict of interest relevant to this article was reported.
References
- 1.Hayreh SS. Prevalent misconceptions about acute retinal vascular occlusive disorders. Prog Retin Eye Res. 2005;24:493–519. doi: 10.1016/j.preteyeres.2004.12.001. [DOI] [PubMed] [Google Scholar]
- 2.Wong TY, Larsen EK, Klein R, et al. Cardiovascular risk factors for retinal vein occlusion and arteriolar emboli: the Atherosclerosis Risk in Communities & Cardiovascular Health studies. Ophthalmology. 2005;112:540–547. doi: 10.1016/j.ophtha.2004.10.039. [DOI] [PubMed] [Google Scholar]
- 3.Mitchell P, Smith W, Chang A. Prevalence and associations of retinal vein occlusion in Australia: the Blue Mountains Eye Study. Arch Ophthalmol. 1996;114:1243–1247. doi: 10.1001/archopht.1996.01100140443012. [DOI] [PubMed] [Google Scholar]
- 4.Klein R, Klein BE, Moss SE, Meuer SM. The epidemiology of retinal vein occlusion: the Beaver Dam Eye Study. Trans Am Ophthalmol Soc. 2000;98:133–141. [PMC free article] [PubMed] [Google Scholar]
- 5.Klein R, Moss SE, Meuer SM, Klein BE. The 15-year cumulative incidence of retinal vein occlusion: the Beaver Dam Eye Study. Arch Ophthalmol. 2008;126:513–518. doi: 10.1001/archopht.126.4.513. [DOI] [PubMed] [Google Scholar]
- 6.Cugati S, Wang JJ, Rochtchina E, Mitchell P. Ten-year incidence of retinal vein occlusion in an older population: the Blue Mountains Eye Study. Arch Ophthalmol. 2006;124:726–732. doi: 10.1001/archopht.124.5.726. [DOI] [PubMed] [Google Scholar]
- 7.The Branch Vein Occlusion Study Group. Argon laser photocoagulation for macular edema in branch vein occlusion. Am J Ophthalmol. 1984;98:271–282. doi: 10.1016/0002-9394(84)90316-7. [DOI] [PubMed] [Google Scholar]
- 8.Chang MA, Fine HF, Bass E, et al. Patients' preferences in choosing therapy for retinal vein occlusions. Retina. 2007;27:789–797. doi: 10.1097/IAE.0b013e31802c0a34. [DOI] [PubMed] [Google Scholar]
- 9.McIntosh RL, Mohamed Q, Saw SM, Wong TY. Interventions for branch retinal vein occlusion: an evidence-based systematic review. Ophthalmology. 2007;114:835–854. doi: 10.1016/j.ophtha.2007.01.010. [DOI] [PubMed] [Google Scholar]
- 10.Scott IU, Ip MS, VanVeldhuisen PC, et al. A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with standard care to treat vision loss associated with macular Edema secondary to branch retinal vein occlusion: the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) study report 6. Arch Ophthalmol. 2009;127:1115–1128. doi: 10.1001/archophthalmol.2009.233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Campochiaro PA, Heier JS, Feiner L, et al. Ranibizumab for macular edema following branch retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology. 2010;117:1102–1112.e1. doi: 10.1016/j.ophtha.2010.02.021. [DOI] [PubMed] [Google Scholar]
- 12.Haller JA, Bandello F, Belfort R, Jr, et al. Dexamethasone intravitreal implant in patients with macular edema related to branch or central retinal vein occlusion twelve-month study results. Ophthalmology. 2011;118:2453–2460. doi: 10.1016/j.ophtha.2011.05.014. [DOI] [PubMed] [Google Scholar]
- 13.Rogers SL, McIntosh RL, Lim L, et al. Natural history of branch retinal vein occlusion: an evidence-based systematic review. Ophthalmology. 2010;117:1094–1101.e5. doi: 10.1016/j.ophtha.2010.01.058. [DOI] [PubMed] [Google Scholar]
- 14.Guthoff R, Meigen T, Hennemann K, Schrader W. Comparison of bevacizumab and triamcinolone for treatment of macular edema secondary to branch retinal vein occlusion in a pair-matched analysis. Ophthalmologica. 2010;224:319–324. doi: 10.1159/000313304. [DOI] [PubMed] [Google Scholar]
- 15.Ehrlich R, Ciulla TA, Moss AM, Harris A. Combined treatment of intravitreal bevacizumab and intravitreal triamcinolone in patients with retinal vein occlusion: 6 months of follow-up. Graefes Arch Clin Exp Ophthalmol. 2010;248:375–380. doi: 10.1007/s00417-009-1211-6. [DOI] [PubMed] [Google Scholar]
- 16.Cekic O, Cakir M, Yazici AT, et al. A comparison of three different intravitreal treatment modalities of macular edema due to branch retinal vein occlusion. Curr Eye Res. 2010;35:925–929. doi: 10.3109/02713683.2010.496540. [DOI] [PubMed] [Google Scholar]