

Abstract
This study evaluated the stretching and dilatation of venous segments ex vivo in subjects with primary varicose veins in comparison with comparable segments from subjects that used the supplement Pycnogenol (150 mg/d) for 3 months before surgery. Subjects with varicose veins and chronic venous insufficiency voluntarily used Pycnogenol for a period of at least 3 months. The segments of veins removed with surgery (in 30 subjects that had used Pycnogenol and in 10 comparable control subjects that had not used the supplement) were compared with normal, unused vein segments harvested for bypass grafting. The segments were suspended and a weight was attached to the distal part of the veins for 3 minutes and dilated with pressurized water. Digital images were recorded; the veins were measured before and after stretching to evaluate elongation. The manipulation of the vein segment was minimal. Tests were completed within 20 minutes after harvesting the veins. All segments were 4 cm long. The stretching test indicated a significantly higher level of passive elongation in control, varicose segments (2.29; 0.65 mm) in comparison with 1.39; 0.2 mm in vein segments from Pycnogenol-using patients. The dilation test showed an average higher dilation (2.19; 0.3 mm) in control varicose veins in comparison with varicose veins from Pycnogenol-using patients (1.32; 0.7 mm) (p < 0.05). Stretching and dilatation were lower in veins from Pycnogenol-using subjects (p < 0.05). The measurement of destretching and the recovery after dilatation indicated a better tone and recovery of the original size/shape in varicose segments from patients using Pycnogenol. Varicose segments had a more significant persistent dilatation and elongation in comparison with normal vein segments. Pycnogenol seems to decrease passive dilatation and stretching and gives vein walls a greater tonic recovery and elasticity that allows the vein to recover its original shape after dynamic stresses.
Keywords: Pycnogenol, chronic venous insufficiency, venous tone, varicose veins
Vascular tone indicates the degree of constriction in a blood vessel relative to its maximally dilated state. Arteries and veins under basal conditions exhibit some degree of tonic basal smooth muscle contraction that determines the diameter and tone of the vessel.1 Basal vascular tone differs among organs according to physiological conditions (i.e., during effort). Organs having a large vasodilatory capacity (e.g., myocardium, skeletal muscle, skin, and splanchnic circulation) have a higher basal vascular tone while organs having relatively low vasodilatory capacity (e.g., cerebral and renal circulations) tend to have a lower vascular tone.
Vascular tone1 2 3 4 5 6 considering physiological condition is determined by the balance of competing vasoconstrictor and vasodilator influences. Extrinsic factors (neurohumoral) such as sympathetic nerves and circulating angiotensin II tend to increase the vascular tone, causing vasoconstriction. Some circulating factors (e.g., atrial natriuretic peptide) decrease vascular tone. Intrinsic factors include the following:
Myogenic mechanisms originating from vascular smooth muscle, which tend to increase tone.
Endothelial factors, such as nitric oxide and endothelin, can either decrease or increase tone, respectively.
Local hormones and chemical substances (e.g., arachidonic acid metabolites, histamine, and bradykinin) can either increase or decrease the vascular tone.
Metabolic by-products or hypoxia generally decrease tone.
The mechanisms by which these influences produce constriction or relaxation of blood vessels involve a variety of signals that change functions and actions of smooth muscles. Venous tone is associated to several factors (quantity of blood present in the system, flow, heart activity, exercise, etc.) and to anatomical alterations (varicosity).
Venous tone of the veins of the legs that bear the full effects of gravity is different from tone in other veins. In chronic venous insufficiency (CVI),3 4 5 6 7 8 venous tone seems to be severely altered particularly in late stages.
The prospective evaluation of venous tone and its variations in CVI may offer a model to study and quantify the effects of treatments on tone2 3 4 5 6 that can be assessed with several methods (air plethysmography, straingauge plethysmography, and laser Doppler, by evaluating the venoarteriolar response or vein wall perfusion).7 8 9 10 11 12
The venous tone model can be applied ex vivo on segments of vein dissected during vein surgery for varicose veins. Vein segments can be filled with water at high pressure (30–80 mm Hg) to test dilatation or suspended with a small weight for minutes to test for elongation. The vein stretches with the action of the weight, and in defined time and conditions, the elongation due to stretching can be measured. Dilatation can be evaluated by passive filling with pressurized water. Dilatation and stretching are more important in varicose veins than in “normal” vein segments.10 11 12 13
This model could be used to evaluate the protective effects on the vein wall of treatments and supplements that may improve venous tone.7 8 9 10
Pycnogenol (Horphag Research, Geneva, Switzerland) is a standardized extract from French pine bark used in the recent past for several vein studies.14 15 16 17 18 19 20 21 22 23 24 25 26 The product is very effective as 100 mg produce significant effects on edema and signs of CVI.24 Pycnogenol is very effective in acute venous edema21 22 with a selective action on lower limb swelling and edema. Pycnogenol has improved venous tone in clinical studies.14 15 16 17 18 19 Pycnogenol improves healing of venous ulcers25 26 and is very effective in CVI in postthrombotic limbs.16
The aim of this study was the evaluation ex vivo of the passive stretching and dilatation of venous segments in subjects with primary varicose veins in comparison with comparable subjects that had used Pycnogenol before surgery for 3 months.
Materials and Methods
Subjects with primary varicose veins and CVI27 (evening swelling, dischromic changes at the perimalleolar region) were included while waiting for surgery. Three groups of veins were compared
Group 1: Patients using the Supplement
For a period of at least 3 months they used elastic stockings and Pycnogenol to control the signs/symptoms of edema, heavier legs or moderate pain after prolonged standing present in all subjects. Below-knee Sigvaris (Sigvaris Management AG, Winterthur, Switzerland) stockings were used as the standard compression. These stockings have a mild-to-moderate compression (14–22 mm Hg at the ankle).
Group 2: Control Veins
Comparable varicose veins segments were collected from patients that did not use the supplement, only the same stockings in the preoperative period.
Groups 3: Normal Veins
This group of nonvaricose vein segments27 was collected after surgery for coronary bypass grafts (unused vein segments).
The CEAP classification9 of these patients was: C4 for varicose veins, edema, initial pigmentation; Ep for primary varicose veins; As2 for superficial veins including the greater saphenous vein mainly above knee; and Pr for reflux. Dilated, varicose veins were considered of surgical interest as they were proximal (above knee), associated with the long saphenous vein and related to signs and symptoms. Veins were prominent and at risk for thrombosis or hemorrhage in case of traumas.27 Subjects had no history of previous treatments (surgery or sclerotherapy), no previous thrombosis or thrombophlebitis and no other disease, metabolic condition or risk factor was present at inclusion. Subjects did not use any drug or other supplement.
Diagnostic Evaluation: Color Duplex
The venous system was evaluated7 8 9 27 with color duplex (Preirus, Hitachi, Japan). The sapheno—femoral and posterior sapheno—popliteal junctions were evaluated for competence with the patient standing. Also perforating veins and incompetent varicose segments were scanned and photographically recorded. Duplex excluded incompetence of the deep venous systems. Any other vascular pathology was excluded.
Surgery
Surgery was performed with spinal anesthesia. Only incompetent segments—defined according to duplex ultrasound findings—of veins were excised.27 28 29 When a useful segment of the long saphenous vein at least 4 cm long—basically cylindrical in shape—was available after surgery. The segment was harvested for the study; it was treated with a careful no-touch technique, without using tweezers. The vein was placed in 34°C saline. The preparation consisted of the atraumatic ligation before excision (3–0 Dexon) of the two extremities. All collaterals were ligated (4–0) or sutured with very small suture (Gore Tex suture CV6; Gore Text, Flagstaff, AZ) under magnification.
The “normal” vein segments were obtained by segments that constituted residual parts, comparable to the varicose vein segments, obtained from unused segments of veins available from veins harvested for coronary bypass grafts. Five samples were made available and used for comparative measurements.
Stretching Test
The vein segments (all cut at 4 cm) were suspended (with saline inside the venous space at 30 mm Hg to keep the vein turgid and with a circular section). Veins without low-pressure saline inside them tend to assume a ribbon-like shape. The vein was suspended and a 10 g weight was attached to the distal part of the vein for 3 minutes. Digital images were recorded, and the images before and after stretching were measured to evaluate elongation. The experiment was conducted only once (Fig. 1).
Fig. 1.
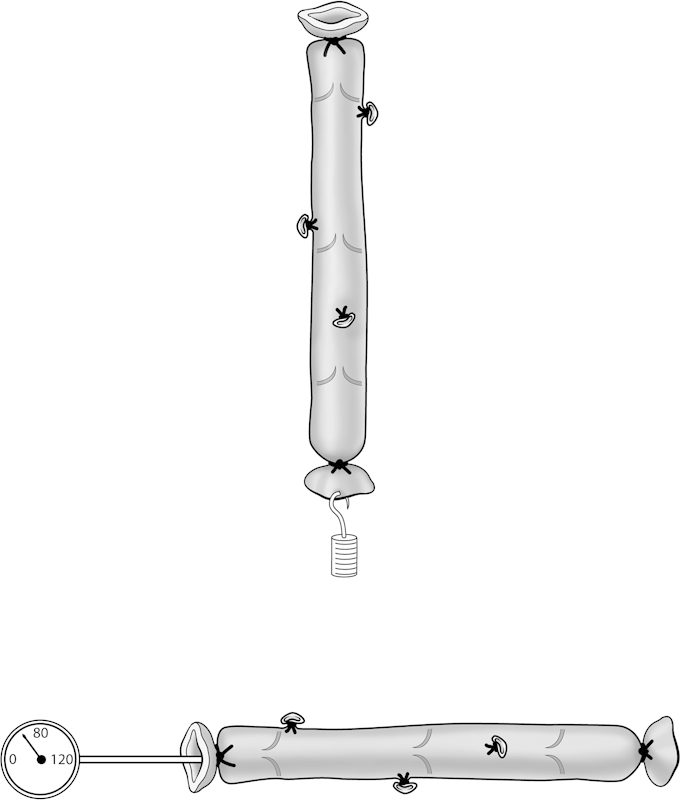
The two tests on the venous segments (stretching and dilatation to pressure).
For the dilatation test the measurement equipment consisted of a pressure gauge linked to a small silicon catheter that allowed the introduction of pressurized water. The vein walls were ligated around the catheter to create a close endovenous space. The pressure (80 mm Hg) was maintained for 3 minutes only; the vein was placed on a glass plate with saline. Manipulation of the vein segment was minimal. During the tests the temperature of the specimens was kept between 31 and 36°C. All tests were completed within 20 minutes after harvesting the vein to avoid the effects of longer preservation on venous tone. Pictures (perpendicular to the vein axis) were measured in postprocessing from the digital images against micrometric scale (the digital pictures measurements were made with a cross-hair system using Adobe Photoshop [Adobe Systems Incorporated, San Jose, CA]).
When 10 control varicose veins and 30 vein segments from patients using Pycnogenol were satisfactorily measured for stretching and dilatation, the study was completed; 56 segments were available, but for various anatomical reasons including vein irregularities, bifurcations, noncylindrical shape, and too many collaterals and sutures, 16 segments were excluded. The samples were weighted on a micrometric scale (Tomopol s100; tomopol GmbH, Lindlar, Germany). Results were coupled (one control vein segment and three comparable Pycnogenol-supplemented vein segments) for their best similarity in weight to have the most comparable variations. Being of the same length and size coupling segments for the most similar weight reduces the possibility of differences in stretching and dilating due to different structures (i.e., wall thickness). Also “normal” veins were matched for weight. Pycnogenol supplementation consisted of 150 mg (three 50 mg tablets were given daily).
The age range of the patients was between 35 and 45 years. This venous tone model,2 28 29 30 31 32 was established by Zukowski et al and more recently by Clarke et al at St Mary's Hospital, Academic Surgical Unit at the Irvine laboratories (UCL, London).33 34 35 36 37 38 39
All patients gave informed consent to the surgical procedures according to the Helsinki declaration. The postsurgical evaluation was part of a diagnostic test—to which patient consented—used to detect possible differences in the elasticity and tone of varicose veins with the aim of forecasting future varicosity recurrence and to suggest appropriate treatments. Pycnogenol was voluntarily assumed as a supplement. This was a noninterventional, supplement study. The bypass vein segments were not collected on purpose for this study but leftovers from surgery were going to be destroyed.
Statistics
At least 10 subjects in each group (control or Pycnogenol) were considered necessary to evaluate differences after at least 3 months of supplementation on the basis of observations from previous studies.
Analysis of variance was used to compare the two main measurements of stretching and dilatation of the varicose segments with the “normal” vein segments. All measurements (variation between the two groups of varicose veins) were considered nonparametric; their differences were evaluated with a nonparametric test (Mann-Whitney). SigmaPlot (Systat Software, Inc., San Jose, CA) software was used to perform all statistical analyses.
Results
The vein segments were excised from 10 separate control subjects (age 38.6; 3.3; 7 females) and 30 separate Pycnogenol subjects (age 38.3; 6.3; 6 females). The normal vein segments were harvested form bypass surgery patients (age 46.7; 3.5; 2 females). One segment corresponded to one patient. The two groups of varicose veins were comparable for age, sex, and clinical distribution (including the anatomy of the veins). All vein segments were from an above-knee segment of greater saphenous vein of less than 35 cm distal to the sapheno–femoral junction. Pycnogenol subjects used the supplements for an average of 93 days (range 77–106) according to the waiting time needed for surgery. No side effects from Pycnogenol were observed. There were no tolerability problems with Pycnogenol.
Measurements
As a reference for normal veins, the stretching test indicated an average increase of 1.13; 0.3 mm and a maximum average dilatation of 1.11; 0.2 mm (Table 1). After releasing the dynamic stress the vein segments recovered partially the initial length and diameter indicating a residual tone of the vein wall able to bring the vein shape to the initial sampling sizes.
Table 1. Increase in maximum length (on stretching), maximum diameter (on pressure dilatation): also the increased residual length after the end of the stretching period and the final residual dilatation when pressure is no longer applied are shown (all measurements are expressed in mm).
| Normal veins | Control varicose veins | Varicose veins pycnogenol |
|
|---|---|---|---|
| Number of patients | 5 | 10 | 30 |
| Stretching | 1.13; 0.3 | 2.29; 0.65a | 1.39; 0.2 |
| Dilatatation | 1.11; 0.2 | 2.19; 0.3a | 1.32; 0.7b |
| Final length after destretching | +0.7; 0.2 | +1.89a | +1.09; 0.2 |
| Final diameter (postdilatation) | +0.2; 0.1 | +1.79a | +0.5; 0.2b |
Note: The numbers are differences before and after stretching of dilating and after the end of stretching and the end of dilatation. All segments of veins were exactly 4 cm at the beginning of the dynamic tests.
Mann-Whitney U test: control veins (values vs. the two other groups); p < 0.05.
ANOVA: evaluation of differences between normal veins and veins from Pycnogenol-supplemented subjects; p < 0.05.
The stretching test in varicose veins indicated a significantly higher level of stretching in control vein segments (2.29; 0.65 mm in comparison with 1.39; 0.2 mm in vein segments from the Pycnogenol-treated group; p < 0.05). The dilatation test showed an average higher dilatation of 2.19; 0.3 mm in comparison with 1.32; 0.7 mm in controls. Therefore, stretching and dilatation were significantly higher in segments from non-Pycnogenol subjects.
Recovery Measurements after Dynamic Stresses
Destretching (return to original size after removing the weight, waiting for 5 minutes) resulted in a decrease in length of the vein segment. At 5 minutes the Pycnogenol vein segments were on average 1.2; 0.43 mm shorter (from the maximum length reached on stretching) (Table 1). Destretching decreased the acquired length (median 44.54%) indicating a residual elasticity. The decrease in endovenous pressure to 30 mm Hg after 5 minutes produced a decrease in the maximum diameter (median decrease 77.16%).
In control vein segments there was a significantly lower destretching (0.4; 0.1 mm) and the dilatation decreased only 0.4; 0.1 mm from the maximum dilatation.
These values were significantly different from the Pycnogenol-supplemented vein segments (p < 0.05). The decreased level of passive stretching and dilatation and the recovery in a few minutes after the dynamic stress indicated that Pycnogenol-supplemented vein segments are more “tonic” and able to passively respond to dynamic stresses. Values are more similar to values in normal segments in comparison with control segments.
Discussion
Venous tone28 29 30 31 is severely altered in varicose veins. Veins show a decrease in elasticity with a lower resistance to dilatation that becomes mainly passive1 2 and is not linked to an effective elastic response to dynamic stresses. Varicose veins do not regain their original dimensions and functions, including the valvular functional capacity, after stretching and dilatation.
Dilatation of venous segments—that is, due to chronic increase in venous pressure—produces a relative incompetence of the valvular cusps. The blood column is not interrupted anymore and the full power and weight of the blood column tends to put pressure on distal valvular elements and vein segments that also became incompetent.
The effect of elastic compression on venous tone in patients with varicose veins has been evaluated with a complex model2 at the Irvine Laboratory (St. Mary's Hospital Medical School, London). Elastic compression and changes in venous wall elasticity were studied in varicose veins simultaneously measuring venous volume and pressure. While the venous outflow was obstructed, the pressure/volume (P/V) relationship of the venous system of the leg was studied and the elastic modulus was calculated. Measurements were made before and after the use of elastic stockings for 6 weeks.31 32 33 34 35 36 37 38 39 Significant improvements were noted in the P/V curve-derived elastic modulus with stockings.8 33 34 35 36 The limbs with varicose veins could be divided into two groups based on the response of the P/V curves to stockings and the severity of disease. Limbs with milder disease shifted their P/V curves toward a more normal pattern. Limbs with severe disease showed evidence of improvement at low but not at high venous pressures. This observation indicated that there is a loss of elasticity and elastic response in most varicose veins. Treatments—that is, compression—can improve elasticity and tone in some patients.8 The observation that the loss of elasticity and tone can be partially corrected suggested the use of Pycnogenol (as a supplement) to produce positive changes in this ex vivo anatomical/physiological study.
According to the present study the reason for the difference of elasticity between pretreated and untreated vein segments could be seen in the inhibition of matrix-degrading enzymes produced by Pycnogenol. The extract and its active metabolite inhibit the matrix metalloproteases in in vitro studies and in human samples.40 Especially, the inhibition of the elastin-degrading elastases helps to keep the venous wall elastic. The action of Pycnogenol on smooth muscles (particularly increased elasticity and increase in resistance to degrading conditions)40 41 42 43 is still under investigation. It seems that Pycnogenol—and its metabolites—may modulate smooth muscle cells activity40 avoiding excess of contraction or passive elongation. Pycnogenol includes 85% proanthocyanidins, 10% organic acids (including caffeine and gallic acid), and 5% water.
Conclusions
The study indicated that varicose veins in subjects using Pycnogenol appear more resistant to dynamic stresses (stretching and dilatation), and that after the stress, recovery to the initial shape, volumes, and sizes can be achieved faster and better. Several potential positive actions of Pycnogenol have been shown in clinical studies on venous disorders and generally on the vascular wall.14 15 16 17 18 19 20 Previous studies had shown that Pycnogenol is incorporated into the venous wall,14 19 and it is possible that its activity on venous tone (as indicated in the present study) may be effective in several other aspects and conditions in the evolution of CVI.
It is possible that a preventive action in earlier stages may make veins more resistant to dilatation and more effective in their response to dynamic stresses.
With Pycnogenol supplementation some varicose veins—at earlier stages—may reduce the rate of progression to CVI. Data from venous studies and from studies on postthrombotic patients indicated the efficacy of Pycnogenol in these conditions. This study may offer an interesting explanation of the effects of Pycnogenol in venous insufficiency. Prospective studies in vivo concerning venous tone are in progress.
In conclusion, the value obtained with Pycnogenol-treated veins after 3 months of supplementation are more similar to the average data obtained with normal vein segments. Pycnogenol seems to decrease the passive dilatation and stretching and to give vein walls a greater power of tonic recovery and elasticity that allows the vein segment to recover its original shape after dynamic stresses.
References
- 1.Caro C G, Pedley T J, Schroter R C, Seed W A. Cambridge: Cambridge University press; 2011. The Mechanics of the Circulation. [Google Scholar]
- 2.Szendro G, Veller M, Fisher C. et al. The effect of elastic compression on the venous tone in patients with varicose veins. Vasa. 1992;21(2):198–202. [PubMed] [Google Scholar]
- 3.Belcaro G, Cesarone M R, de Sanctis M T. et al. Laser Doppler and transcutaneous oximetry: modern investigations to assess drug efficacy in chronic venous insufficiency. Int J Microcirc Clin Exp. 1995;15 01:45–49. doi: 10.1159/000179095. [DOI] [PubMed] [Google Scholar]
- 4.Petruzzellis V, Troccoli T, Candiani C. et al. Oxerutins (Venoruton): efficacy in chronic venous insufficiency—a double-blind, randomized, controlled study. Angiology. 2002;53(3):257–263. doi: 10.1177/000331970205300302. [DOI] [PubMed] [Google Scholar]
- 5.Bertrand-Thiebault C, Ferrari L, Boutherin-Falson O. et al. Cytochromes P450 are differently expressed in normal and varicose human saphenous veins: linkage with varicosis. Clin Exp Pharmacol Physiol. 2004;31(5-6):295–301. doi: 10.1111/j.1440-1681.2004.03996.x. [DOI] [PubMed] [Google Scholar]
- 6.Svedman C, Cherry G W, Ryan T J. The veno-arteriolar reflex in venous leg ulcer patients studied by laser Doppler imaging. Acta Derm Venereol. 1998;78(4):258–261. doi: 10.1080/000155598441819. [DOI] [PubMed] [Google Scholar]
- 7.Belcaro G, Nicolaides A N, Stansby G. London: Imperial College Press; 2001. The Venous Clinic. [Google Scholar]
- 8.Belcaro G, Veller M, Nicolaides A N. London: Saunders; 1999. Venous Disorders. A Manual of diagnosis and Treatment. [Google Scholar]
- 9.Belcaro G, Nicolaides A N. London: Imperial College Press; 2001. Non invasive investigations in vascular disease. [Google Scholar]
- 10.Belcaro G, Hofman U, Bollinger A, Nicolaides A N. London: MedOrion; 1996. Laser Doppler. [Google Scholar]
- 11.Belcaro G Taccoen A Venous wall perfusion London: International Union of Angiology; 1197. Abstract 122 [Google Scholar]
- 12.Belcaro G, Laurora G, Cesarone M R. et al. Vasa vasorum visualised by power-Doppler in normal and arteriosclerotic carotid arteries. Vasa. 1996;25(3):226–232. [PubMed] [Google Scholar]
- 13.Taccoen A, Belcaro G, Lebard C, Zuccarelli F. Etiologies et mécanismes des varices: réalités et perspectives. Sang Thrombose Vaisseau. 1997;9:354–363. [Google Scholar]
- 14.Belcaro G, Hu S, Hosoi M. Circulation Sciences. Pycnogenol into the venous wall. Physiology and chromatography. Circulation Sciences Journal. 2010;13:18. [Google Scholar]
- 15.Belcaro G, Cesarone M R, Errichi B M. et al. Venous ulcers: microcirculatory improvement and faster healing with local use of Pycnogenol. Angiology. 2005;56(6):699–705. doi: 10.1177/000331970505600607. [DOI] [PubMed] [Google Scholar]
- 16.Errichi B M, Belcaro G, Hosoi M. et al. Prevention of post thrombotic syndrome with Pycnogenol® in a twelve month study. Panminerva Med. 2011;53(3) 01:21–27. [PubMed] [Google Scholar]
- 17.Nuzum D S Gebru T T Kouzi S A Pycnogenol for chronic venous insufficiency Am J Health Syst Pharm 201168171589–1590., 1599–1601 [DOI] [PubMed] [Google Scholar]
- 18.Cesarone M R, Belcaro G, Rohdewald P. et al. Improvement of signs and symptoms of chronic venous insufficiency and microangiopathy with Pycnogenol: a prospective, controlled study. Phytomedicine. 2010;17(11):835–839. doi: 10.1016/j.phymed.2010.04.009. [DOI] [PubMed] [Google Scholar]
- 19.Cesarone M R, Belcaro G, Rohdewald P. et al. Rapid relief of signs/symptoms in chronic venous microangiopathy with pycnogenol: a prospective, controlled study. Angiology. 2006;57(5):569–576. doi: 10.1177/0003319706291392. [DOI] [PubMed] [Google Scholar]
- 20.Belcaro G, Cesarone M R, Ricci A. et al. Control of edema in hypertensive subjects treated with calcium antagonist (nifedipine) or angiotensin-converting enzyme inhibitors with Pycnogenol. Clin Appl Thromb Hemost. 2006;12(4):440–444. doi: 10.1177/1076029606292248. [DOI] [PubMed] [Google Scholar]
- 21.Belcaro G, Cesarone M R, Rohdewald P. et al. Prevention of venous thrombosis and thrombophlebitis in long-haul flights with pycnogenol. Clin Appl Thromb Hemost. 2004;10(4):373–377. doi: 10.1177/107602960401000410. [DOI] [PubMed] [Google Scholar]
- 22.Cesarone M R, Belcaro G, Nicolaides A N. et al. Prevention of venous thrombosis in long-haul flights with Flite Tabs: the LONFLIT-FLITE randomized, controlled trial. Angiology. 2003;54(5):531–539. doi: 10.1177/000331970305400502. [DOI] [PubMed] [Google Scholar]
- 23.Boisseau M R. Pharmacological targets of drugs employed in chronic venous and lymphatic insufficiency. Int Angiol. 2002;21(2) 01:33–39. [PubMed] [Google Scholar]
- 24.Cesarone M R, Belcaro G, Rohdewald P. et al. Comparison of Pycnogenol and Daflon in treating chronic venous insufficiency: a prospective, controlled study. Clin Appl Thromb Hemost. 2006;12(2):205–212. doi: 10.1177/107602960601200209. [DOI] [PubMed] [Google Scholar]
- 25.Belcaro G, Cesarone M R, Errichi B M. et al. Venous ulcers: microcirculatory improvement and faster healing with local use of Pycnogenol. Angiology. 2005;56(6):699–705. doi: 10.1177/000331970505600607. [DOI] [PubMed] [Google Scholar]
- 26.Vinciguerra G, Belcaro G, Cesarone M R. et al. Cramps and muscular pain: prevention with pycnogenol in normal subjects, venous patients, athletes, claudicants and in diabetic microangiopathy. Angiology. 2006;57(3):331–339. doi: 10.1177/000331970605700309. [DOI] [PubMed] [Google Scholar]
- 27.Doherty G M. New York, NY: McGraw Hill; 2003. Current Surgical Diagnosis and Treatment, 12th ed. [Google Scholar]
- 28.Nicolaides A N; Cardiovascular Disease Educational and Research Trust; European Society of Vascular Surgery; The International Angiology Scientific Activity Congress Organization; International Union of Angiology; Union Internationale de Phlebologie at the Abbaye des Vaux de Cernay. Investigation of chronic venous insufficiency: A consensus statement (France, March 5-9, 1997) Circulation 200010220E126–E163. [DOI] [PubMed] [Google Scholar]
- 29.Kasperczak J, Ropacka-Lesiak M, Breborowicz H G. Definition, classification and diagnosis of chronic venous insufficiency - part II [in Polish] Ginekol Pol. 2013;84(1):51–55. doi: 10.17772/gp/1540. [DOI] [PubMed] [Google Scholar]
- 30.Ropacka-Lesiak M, Kasperczak J, Breborowicz G H. Risk factors for the development of venous insufficiency of the lower limbs during pregnancy—part 1 [in Polish] Ginekol Pol. 2012;83(12):939–942. [PubMed] [Google Scholar]
- 31.Somers P, Knaapen M. The histopathology of varicose vein disease. Angiology. 2006;57(5):546–555. doi: 10.1177/0003319706293115. [DOI] [PubMed] [Google Scholar]
- 32.Thulesius O. London: Saunders; 1999. Physiology of veins and their relationship with venous disorders. [Google Scholar]
- 33.Clarke G H. London: University College; 1989. Venous Elasticity [dissertation] [Google Scholar]
- 34.Beckwith T Clarke G H Richardson G A Correlation between blood flow volume and ultrasonic Doppler wave forms in the study of valve efficiency In: Intern Union Phlebologie International Union of Angiology (London)1991. Abstract 23 [Google Scholar]
- 35.Clarke H, Smith S RG, Vasdekis S N, Hobbs J T, Nicolaides A N. Role of venous elasticity in the development of varicose veins. Br J Surg. 1989;76(6):577–580. doi: 10.1002/bjs.1800760617. [DOI] [PubMed] [Google Scholar]
- 36.Clarke G H, Vasdekis S N, Hobbs J T, Nicolaides A N. Venous wall function in the pathogenesis of varicose veins. Surgery. 1992;111(4):402–408. [PubMed] [Google Scholar]
- 37.Hosoi Y, Zukowski A, Kakkos S K, Nicolaides A N. Ambulatory venous pressure measurements: new parameters derived from a mathematic hemodynamic model. J Vasc Surg. 2002;36(1):137–142. doi: 10.1067/mva.2002.124622. [DOI] [PubMed] [Google Scholar]
- 38.Zukowski A J, Nicolaides A N, Szendro G. et al. Haemodynamic significance of incompetent calf perforating veins. Br J Surg. 1991;78(5):625–629. doi: 10.1002/bjs.1800780532. [DOI] [PubMed] [Google Scholar]
- 39.Nicolaides A N, Zukowski A J. The value of dynamic venous pressure measurements. World J Surg. 1986;10(6):919–924. doi: 10.1007/BF01658640. [DOI] [PubMed] [Google Scholar]
- 40.Grimm T, Schäfer A, Högger P. Antioxidant activity and inhibition of matrix metalloproteinases by metabolites of maritime pine bark extract (pycnogenol) Free Radic Biol Med. 2004;36(6):811–822. doi: 10.1016/j.freeradbiomed.2003.12.017. [DOI] [PubMed] [Google Scholar]
- 41.Grimm T, Chovanová Z, Muchová J. et al. Inhibition of NF-kappaB activation and MMP-9 secretion by plasma of human volunteers after ingestion of maritime pine bark extract (Pycnogenol) J Inflamm (Lond) 2006;3:1. doi: 10.1186/1476-9255-3-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Fitzpatrick D F, Bing B, Rohdewald P. Endothelium-dependent vascular effects of Pycnogenol. J Cardiovasc Pharmacol. 1998;32(4):509–515. doi: 10.1097/00005344-199810000-00001. [DOI] [PubMed] [Google Scholar]
- 43.Ivanov V, Ivanova S, Roomi M W, Kalinovsky T, Niedzwiecki A, Rath M. Extracellular matrix-mediated control of aortic smooth muscle cell growth and migration by a combination of ascorbic acid, lysine, proline, and catechins. J Cardiovasc Pharmacol. 2007;50(5):541–547. doi: 10.1097/FJC.0b013e318145148e. [DOI] [PubMed] [Google Scholar]