

The authors conclude that transperitoneal laparoscopic nephropexy with nonabsorbable polymer clips for mobile kidney is a safe and successful procedure.
Keywords: Kidney, Laparoscopy, Mobile kidney, Nephropexy, Polymer clips
Abstract
Background and Objectives:
We present our initial experience and long-term results with transperitoneal laparoscopic nephropexy with nonabsorbable polymer clips.
Methods:
Seven patients aged 34 to 47 years previously diagnosed with mobile kidney presented with chronic pain refractory to analgesics and underwent a transperitoneal laparoscopic nephropexy procedure with nonabsorbable polymer clips by fixing the perirenal tissue to the transversus abdominis fascia and triangular ligament.
Results:
Mean operation time was 20 minutes. All patients were discharged after 24 hours. Follow-up intravenous pyelogram (IVP) at 60 and 150 days showed the right kidneys in a more cephalad position, and showed pelvicaliceal dilatations and that the ureteral kinks seemed to be resolved. On days 15, 60, 90, and 150 of the first- and second-year follow-ups, severity of pain was 1 of 10 on the visual analog scale.
Conclusion:
We believe that the technique of transperitoneal laparascopic nephropexy with nonabsorbable polymer clips on patients with symptomatic mobile kidney is safe and easy to perform and shows successful long-term results.
INTRODUCTION
Nephropexy, the surgical treatment for mobile kidney (nephroptosis), was formerly performed by open procedure. Laparoscopic nephropexy was first described by Urban et al in 1993.1 Surgical objective of nephropexy was to immobilize the kidney in a more cephalad position and prevent the associated obstruction of the renal pelvis, as well as to reduce the tension on the ureter and renal pedicle. Fixation procedures are generally performed in 3 different techniques One of them is using the renal capsula for fixation of kidney. The second is using fascial fleps or muscle bonds for the fixation. The third one is the fixation of kidney with exogenous materials such as clips and tapes.2 In laparoscopic techniques, the capsule of the kidney is sutured to the fascia of the psoas or quadratum lumborum muscles in most cases. Here we present our clinical series with 7 patients who were successfully treated via a transperitoneal laparoscopic approach in which Gerota's fascia and the perirenal fat tissue were attached to the transversus abdominis fascia with nonabsorbable polymer clips (Hem-O-Lok clips, Pilling Weck, Teleflex Medical, Markham, ON, Canada).
MATERIALS AND METHODS
Patients
Between 2006 and 2009, 7 women, ranging in age from 34 to 47 years old (mean age 39.2 years), were referred to our department for surgical repair of a mobile kidney. All had right-sided chronic pain refractory to analgesics, and preoperative workup with intravenous pyelography and CT scan showed a mobile right kidney. Preoperative pain scores using the visual analog scale are shown in Table 1. None of the patients had any history of urinary tract infections, hypertension, or renal calculi. The 7 patients underwent a transperitoneal laparoscopic nephropexy procedure with nonabsorbable polymer clips by fixation of the perirenal tissue to the transversus abdominis fascia and the triangular ligament.
Table 1.
Preoperative and Postoperative Pain Scores and the Operation Times of All Patients
| Patient No. | Age, y | Preoperative VAS | Postoperative VAS | Blood Loss, mL | Operation Time, min |
|---|---|---|---|---|---|
| 1 | 34 | 10/10 | 1/10 | <20 | 15 |
| 2 | 34 | 7/10 | 1/10 | <20 | 25 |
| 3 | 39 | 9/10 | 1/10 | <20 | 22 |
| 4 | 40 | 8/10 | 1/10 | <20 | 25 |
| 5 | 40 | 9/10 | 1/10 | <20 | 20 |
| 6 | 41 | 8/10 | 1/10 | <20 | 20 |
| 7 | 47 | 8/10 | 1/10 | <20 | 18 |
VAS =Visual analog score.
Surgical Technique
A transperitoneal laparoscopic technique, as described by Lee and Clayman, was used.3 The colon was initially reflected medially. The posterior peritoneum was incised and was dissected from Gerota's fascia at the upper pole of the kidney. The Gerota's fascia was then attached to the transversus abdominis fascia and the incised lateral edge of the infrahepatic triangular ligament with nonabsorbable polymer clips (Hem-O-Lok clips, Pilling Weck, Teleflex Medical).
RESULTS
Estimated blood loss was <20 mL in each patient. Mean operation time was 20.7 minutes. None of the patients needed postoperative analgesic medication and they were discharged from the hospital 24 hours after surgery with instructions for bed rest. The patients returned for postoperative follow-up visits on postoperative days 7, 15, 60, 90, and 210. All patients reported improved symptoms after laparoscopic nephropexy. One of the patient's follow-up intravenous pyelogram (IVP) on day 60 is shown in Figure 1B and day 210 is shown in Figure 1C. The follow-up IVP showed that the right kidney was more cephalad relative to its preoperative position by the thickness of 1 vertebra (Figure 1). The dilatation in the collecting system and the kink in the ureter, both visible in the preoperative films, had resolved (Figure 2). On days 15, 60, 90, and 210, the patients described their pain as 1 of 10 on the visual analog scale. No complications were observed in 2 years of follow-up. Patients were asked about the operative outcomes. All patients were satisfied at the 2-year follow-up period. Preoperative and postoperative pain scores and the operation time are given in Table 1.
Figure 1.

A, Preoperative intravenous pyelography. The dilatation in the collecting system and the link in the ureter. B, Postoperative films taken at day 60 after surgery. C, postoperative films taken at day 210 after surgery.
Figure 2.
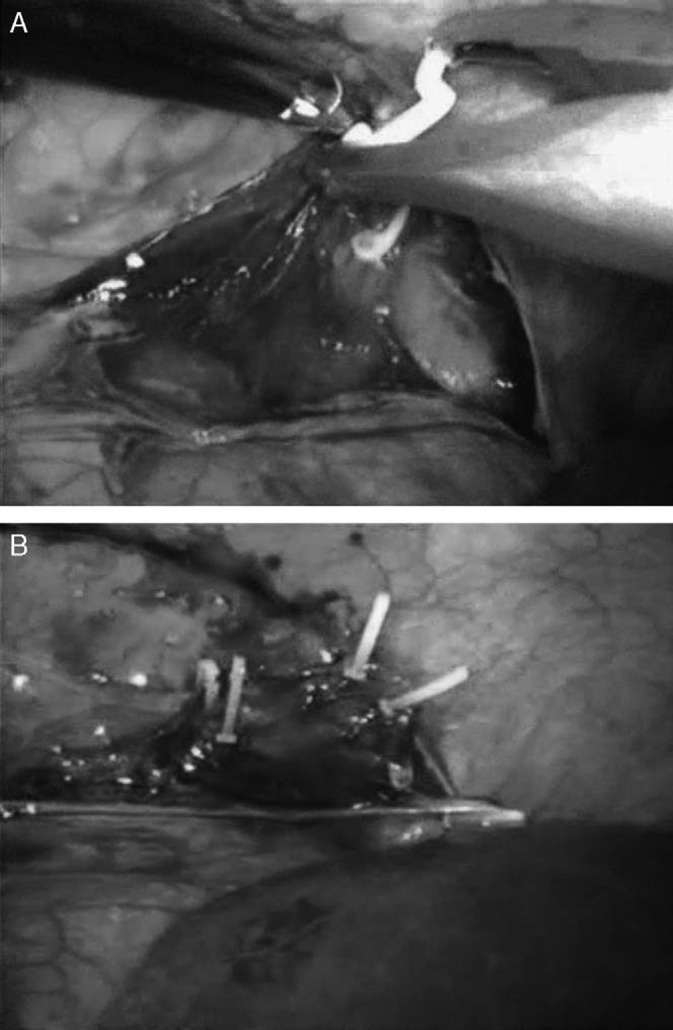
A, Attachment procedure with an polymer clips applicator. B, Gerota's fascia and the perirenal fat tissue was completely attached to the transversus abdominis fascia and triangular ligament with polymer clips.
DISCUSSION
Mobile kidney, also known as nephroptosis, is defined as downward displacement of the kidney by 5 cm when the patient's position is changed from supine to erect.4 The disorder is often present in young and slim women, and the right kidney is most often affected.2–5 It may be asymptomatic or associated with long periods of standing and recurrent urinary tract infections.4 Many operative techniques and modifications of nephropexy have been described, but no definitive procedure exists, and urologists generally have been hesitant to treat mobile kidney because the available treatments, even though most of them are laparoscopic techniques, are invasive, although the symptoms are not always severe.6,7 For patients with mobile kidney, the decision algorithm for treatment involves two general questions: whether surgery should be performed, and, if so, by what method. Surgery is recommended generally for patients who have both symptoms and objective findings because radiologically visible mobile kidney is more common than the symptomatic form of the disease.8 Surgical methods used for treating mobile kidney have ranged from open surgery9 to laparoscopy6,8 to percutaneous treatment.10,11 Open surgery is generally not preferred due to its invasiveness. The percutaneous method offers some advantages, such as short operation time and the ability to be performed using local anesthesia with ultrasonography or fluoroscopy. However, its disadvantages include the lack of visualization of nearby structures that could be damaged during the procedure, as well as a longer hospital stay and postoperative rest period compared with laparoscopy.10 Laparoscopic nephropexy was first reported by Urban et al in 1993 and is likely to remain the mainstay of surgical intervention in the future. It can be performed with either a transperitoneal or retroperitoneal approach. Most authors have used the transperitoneal approach because it provides a larger working space and avoids the lateral position of the patient used in the retroperitoneal approach, in which a mobile kidney can fall forward and become less accessible. Three main surgical techniques for nephropexy have been used with success, and these are fixation using the renal capsule, fixation with fascial flaps or muscle bands, and fixation with foreign material.2 In the patient reported here, Gerota's fascia and perirenal fat tissue were attached to the incised edge of the infrahepatic triangular ligament and to the fascia of the transversus abdominis muscle with nonabsorbable polymer clips (Hem-O-Lok clips, Pilling Weck, Teleflex Medical) (Figure 2). To the best of our knowledge, this technique has not been used previously. In the report by Rassweiler et al12 that described their experience with 200 cases of retroperitoneoscopic surgery, nephropexy was classified as technically difficult. The advantage of the technique reported here is that it is easier and quicker than other techniques. Long-term results were successful. At the 2-year follow-up, our patients had not experienced any recurrence of symptoms, but this possibility of success should be explored in larger series
CONCLUSION
We believe that the technique of transperitoneal laparascopic nephropexy with nonabsorbable polymer clips on patients with symptomatic mobile kidney is easy to perform and shows successful long-term results.
Contributor Information
C̗agri Güneri, Department of Urology, Koru Hospital, Ankara, Turkey..
Lütfi Tunc̗, Department of Urology, Gazi University, Ankara, Turkey..
Mustafa Kirac̗, Department of Urology, Koru Hospital, Ankara, Turkey..
Hasan Biri, Department of Urology, Gazi University, Ankara, Turkey..
Ibrahim Bozkirli, Department of Urology, Gazi University, Ankara, Turkey..
References
- 1. Urban D, Clayman R, Kerbl K, Figenshau RS, McDougall EM. Laparoscopic nephropexy for symptomatic nephroptosis: initial case report. J Endourol. 1993;7:27–30 [DOI] [PubMed] [Google Scholar]
- 2. Harrison LH. Nephropexy. In: Glenn JF, ed. Urological Surgery. 3rd ed Philadelphia: JB Lippincott Co; 1983;253–355 [Google Scholar]
- 3. Lee DI, Clayman RV. Standart transperitoneal and retroperitoneal laparoscopic nephrectomy for clinical T1-3a, N0, and M0 tumors. In: Cadeddue JA, ed. Laparoscopic Urologic Oncology. 1st ed Totowa, NJ: Humana Press, Inc. 2004;3–18 [Google Scholar]
- 4. Thomson WN, Innes JA, Munro JF, Geddes AM, Prescott RJ, Murdoch JM. Renal mobility in women attending a pyelonephritis clinic and in controls. Br J Urol. 1978;50:73–75 [DOI] [PubMed] [Google Scholar]
- 5. Young HH, Davis DM. Malformation and abnormalities of the urogenital tract. In: Saunders WB, ed. Young's Practice of Urology. vol 2 Philadelphia: WB Saunders Co; 1926;1–36 [Google Scholar]
- 6. Matsui Y, Matsuta Y, Okubo K, Yoshimura K, Terai A, Arai Y. Laparoscopic nephropexy: treatment outcome and quality of life. Int J Urol. 2004;11:1–6 [DOI] [PubMed] [Google Scholar]
- 7. Sigel A, Schrett KM. Nephroptose. In: Hohenfellner R, Zingg EJ, eds. Urologie in Klinik und Praxis. vol 2 New York, NY: Thieme; 1983;868 [Google Scholar]
- 8. Elashry OM, Nakada SY, McDougall EM, Clayman RV. Laparoscopic nephropexy: Washington University experience. J Urol. 1995;154:1655–1659 [DOI] [PubMed] [Google Scholar]
- 9. Barber NJ, Thompson PM. Nephroptosis and nephropexy—hung up on the past? Eur Urol. 2004;46:428–433 [DOI] [PubMed] [Google Scholar]
- 10. Khan AM, Holman E, Toth CS. Percutaneous nephropexy. Scand J Urol Nephrol. 2000;34:157–161 [DOI] [PubMed] [Google Scholar]
- 11. Goldfischer ER, Al Kandari AM, Baernardo NO. Percutaneous surgery in a patient with nephroptosis. J Urol. 1999;161:3959915410 [Google Scholar]
- 12. Rassweiler JJ, Seemann O, Frede T, Henkel TO, Alken P. Retroperitoneoscopy: experience with 200 cases. J Urol. 1998;160:1265–1269 [DOI] [PubMed] [Google Scholar]