
Fig. 12.
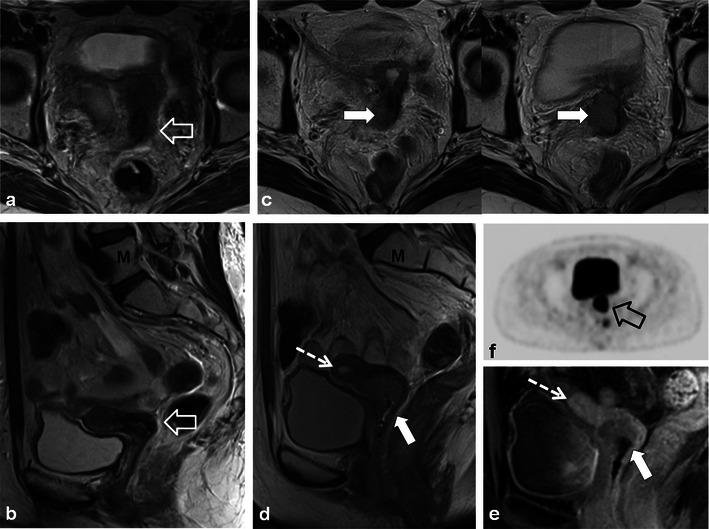
A 56-year-old woman with previous cervical squamous cell carcinoma treated remotely with RT. Post-therapy baseline pelvic MRI demonstrates the normal cervical zonal anatomy with homogeneous low T2 signal intensity (open white arrows) on axial and sagittal T2 TSE (a and b) consistent with complete response and a tumour-free irradiated cervix. Note global uterine atrophy in b commonly seen following pelvic RT. Follow-up pelvic MRI performed 1 year later demonstrates interval development of a well-defined intermediate T2 signal intensity mass in the cervix (closed white arrow) on axial (c) and sagittal (d) T2 TSE. Note interval development of hydrometra (dashed arrow in d) due to the obstructing mass. The mass is characteristically hypovascular in relation to the atrophic uterus after gadolinium injection on sagittal T1 fat saturated GRE image (e). Axial PET image (f) from whole-body 18F-fluorodeoxyglucose (FDG) PET study performed the same day shows corresponding area of avid FDG uptake. The imaging findings are consistent with locally recurrent tumour, which was proven at biopsy