
Figure 2.
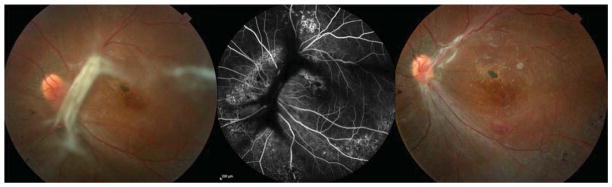
Case 11: A 33-year-old male with sickle cell-hemoglobin C disease developed a progressive tractional retinal detachment in the left eye. Best corrected visual acuity (BCVA) was 20/400. He underwent 25-gauge pars plana vitrectomy (PPV), endolaser to peripheral vitreoretinal proliferation, membrane peeling, and 14% C3F8 gas tamponade. BCVA 2 months after the operation was 20/300, with vision limited by macular atrophy and lamellar hole. Left: A tractional vitreoretinal membrane is involving the nasal and superior macula. There is an epiretinal membrane with lamellar hole. Middle: Fluorescein angiography revealed shadowing of fluorescence from the tractional membrane and areas of hyperfluorescence from multiple window defects, thought secondary to a previous inferior choroidal infarct. Right: Two months after PPV, the traction is released, and the retina is attached; however, BCVA is limited by pre-existing foveal atrophy.