
Figure 4.
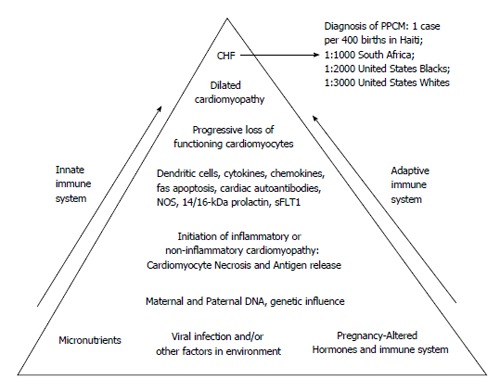
Schematic hypothesis for pathogenesis of peripartum cardiomyopathy. At the base of the pyramid are listed multiple potential contributing factors. Potential viruses include coxsackievirus B3, adenovirus, and parvovirus B19. Dendritic cells are activated by antigen(s) with initiation of a process leading to a cardiomyopathy that may be histologically either inflammatory or non-inflammatory. Cardiomyocyte damage results in the release of previously sequestered cardiac proteins with subsequent production of various autoantibodies, including but not limited to cardiac myosin heavy chain, cardiac Tropin-I, putative cardiac transaldolase), and cardiac beta 1-adrenergic receptor autoantibodies. Production of cytokines, chemokines, nitric oxide synthase (NOS) contribute to the negative inotropic effect. Fas-mediated apoptosis contributes to eventual cardiomyocyte loss. Ultimately, with the progressive loss of functioning cardiomyocytes, dilated cardiomyopathy and congestive heart failure (CHF) ensue, permitting a clinical diagnosis of PPCM. Both inate and adaptive immunity are involved, with participation of both cellular and humoral immune systems. Recently, other potential cardiotoxic substances have been identified, including 14/16 kDa-prolactin metabolites and kinase enzyme system, sFLT1[21,26,28,32,33,37,38,44,63,66,70,77,80,93]. PPCM: Peripartum cardiomyopathy.