

Abstract
Introduction:
Paying attention to improving the nutritional status of adolescents can be one of the most effective fundamental measures for preventing chronic diseases, particularly cardiovascular diseases in later life. Identifying the predicting elements in different behaviors is one of the most effective ways that can be considered in prevention programs in different communities, particularly in developing countries. The purpose of was to determine the perceived efficacy, benefits and barriers related to a healthy nutrition pattern and the relation of these variables with a healthy diet in male and female high school students in Izeh city.
Materials and Methods:
In this cross-sectional descriptive and analytic study conducted throughout high schools in Izeh City, the subjects were 500 students (300 girls and 200 boys) from the 1390-91 school years who were selected through the multistage random sampling method; the acquired data was then studied and analyzed. The data for this study was gathered through a multi-sectional questionnaire (that included demographic characteristics, self-efficacy, perceived benefits and barriers). The Independent t-test, Spearman's Correlation, Pearson's Correlation Coefficient and Linear Regression were used to interpret and analyze the data.
Results:
Data analysis showed that the mean age of male participants was 15.67 ± 0.95 years and females 15.86 ± 1.16 years. The mean score for healthy eating patterns in male students was 46.83 ± 14.86 and in female students 44.20 ± 14.16 respectively. The mean score for perceived benefits of healthy eating in girls was significantly higher than that in boys. There was a direct meaningful relationship between the mean score of benefits and perceived self-efficacy with the healthy eating behaviors in the two sexes, (P < 0.001). The results of the multiple linear regression analysis revealed that the most important predictive factors in the students’ healthy eating behavior are self-efficacy and perceived benefits respectively and that perceived barriers is not an influencing predictor in healthy eating patterns.
Conclusion:
The results of this study showed that many factors influence students’ diet pattern and undeniably the role of these factors are not alike in the two sexes. The results also showed that perceived self-efficacy and benefits of healthy nutrition strengthens healthy eating behavior in students and thus these factors should be considered by health authorities in the country in any future programming.
Keywords: Healthy eating, perceived barriers, perceived benefits, perceived self-efficacy, students
INTRODUCTION
Various studies have emphasized the importance and benefits of healthy nutrition in reducing the risk of many chronic diseases including cardiovascular diseases.[1,2,3]
The World Health Organization in its report has attributed 2.7 million of the total deaths in the world per year to diets low in fruits and vegetables.[4] In Iran a nutritional transition is currently occurring, especially in big cities, and subsequently diet-related chronic diseases are rapidly increasing.[5] Tehran's lipid and glucose study observed a negative trend with respect to the diet quality in children and adolescents compared with the recommendations for preventing cardiovascular diseases.[6] A study among the students of Iran's University of Medical Sciences showed that the amount of daily fat intake is more than the daily calories plus the dietary cholesterol and saturated fat is more than the recommended amount. Besides, a significant difference was observed between the mean dietary fat intake in male and female students in a way that the average consumption was higher in boys than in girls.[7] Another similar study on the students of Iran's University of Medical Sciences showed that the intake of some vitamins, folic acid and pantothenic acid was insufficient compared with the recommended amounts suggested by the RDA (Recommended Dietary Allowances) plus the average daily intake was higher in female students compared to males.[8] In 2003, Motlagh and colleagues conducted a study in various provinces of the country that showed the low frequency of fruit, vegetable and meat substitute (like beans) consumption and the high consumption of snacks between meals containing sweets and candy as well as salty and fatty snacks among Iranian adolescents.[9]
A considerable amount of research has been done worldwide to examine dietary patterns and their relationship with perceived self-efficacy, perceived benefits and perceived barriers;[10,11] however, in developing countries, particularly in our own country studies in this area are poor and insufficient. Thus this study was conducted to determine the perceived benefits, barriers and self-efficacy in predicting dietary behavior in male and female high school students.
MATERIALS AND METHODS
This cross-sectional descriptive analytical study targeted male and female high school students in Izeh City. A sample size level of 500 students, 300 girls and 200 boys, were randomly selected. Students who participated in this study were able to answer all the questions and were not following any special diet due to any specific reason. A questionnaire comprising 54 questions grouped into three sections was utilized for data collection. The questionnaire comprised questions regarding demographic characteristics, healthy eating pattern and questions related to the health belief model. Demographic data consisted of five questions. The questions in the health eating pattern were adopted from the health-promoting lifestyle program survey (HPLP II) that has been time and again approved by different internal and external studies. This section included 12 questions and answers were scored on a four-point Likert scale: 0 never, 1 sometimes, 2 often and 3 regularly. The minimum score for the healthy eating pattern was zero and the maximum, 36. A higher score indicated a healthier diet and a lower score showed poorer nutrition. Cronbach's alpha from the pilot study data regarding healthy nutrition was 0.735.
The self-efficacy for healthy eating questionnaire included 19 questions. The answers were scored on a 5-point Likert scale: I’m not at all sure 0 points, I’m not sure 1 point, I’m somewhat sure 2 points, I’m sure 3 points and I’m extremely sure 4 points. The minimum self-efficacy score for healthy eating was zero and the maximum was 76. A higher score indicated a higher perceived self-efficacy for healthy eating and a lower score showed lower perceived self-efficacy. Cronbach's alpha from the pilot study data regarding self-efficacy for healthy eating was 0.867.
The questionnaire regarding the benefits of and barriers to healthy eating included 18 questions: 9 of which were related to the perceived benefits and 9 to the perceived barriers. Each question had four options ranging from “Completely agree” to “Completely disagree” and was scored zero to 3. The minimum score for perceived benefits of and barriers to healthy eating was zero and the maximum score was 27. A higher score indicated higher perceived barriers and benefits and a lower score showed lower perceived barriers and benefits. Cronbach's alpha from data regarding perceived benefits of and barriers to healthy eating was 0.701.
After the questionnaire was designed, a pilot study was conducted and the test re-test method was used to assess the test reliability in which a 0.735 ratio was achieved for questions regarding healthy eating, 0.867 for questions related to self-efficacy for healthy eating and 0.701 for questions concerning benefits and barriers to healthy eating, respectively.
While designing the questionnaire and scoring the questions, the views of health education specialists were taken into account and after a preliminary study, ambiguous questions were removed and the validity of the questionnaire was approved.
The questionnaire was distributed amongst the target group and completed. The data from the questionnaire was then extracted and inserted into the SPSS 18 software and statistical tests consisting of the Independent T-Test, Spearman's Correlation, Pearson's Correlation Coefficient and Linear Regression were used. The criterion for statistical significance was P < 0.05.
RESULTS
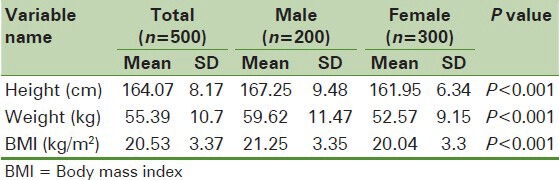
The study was conducted on 500 high school students of whom 300 were girls and 200 were boys. The average age of male participants was 15.67 ± 0.95 years and females 15.86 ± 1.16. The mean height, weight and body mass index in girls was less than boys in a manner that the independent t-test shows a significant difference (P < 0.001). Table 1 shows the mean height, weight and body mass index (BMI) of the sample students according to their gender.
Table 1.
Comparison of demographic variables in female and male students
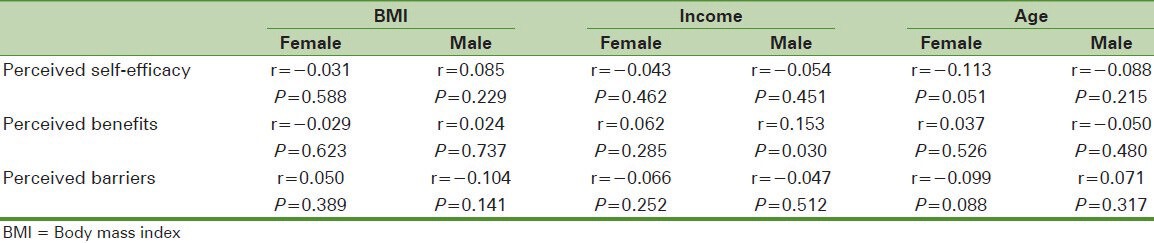
The study indicated that there is no significant association between BMI and the health belief model constructs (self-efficacy, perceived benefits and perceived barriers of healthy eating), based on Spearman's Correlation test.
The study also demonstrated that the family income of the male students has a direct meaningful relationship with the perceived benefits of healthy eating (P = 0.030 and r = 0.153) while in the case of females there was no relationship between the family income and the health belief model constructs examined. According to Pearson's Correlation test there was no significant relationship between the age variable in male and female students, and the constructs of benefits, barriers and perceived self-efficacy aimed towards healthy eating [Table 2].
Table 2.
Relationship between some components of health belief model and demographic variables in female and male students
The mean score for healthy eating behavior in the students surveyed was 45.25 ± 14.48 in which a significant difference was found (P = 0.047) between the dietary behavior score in boys (46.83 ± 14.86) and girls (44.20 ± 14.16).
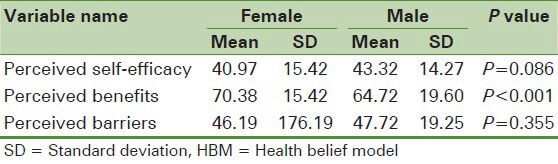
The findings also indicate that the mean score for perceived barriers to healthy eating in male and female students was not significantly different (47.72 and 46.19 respectively). The study's other findings show that the mean score for perceived benefits of healthy eating in female students is significantly higher than in male students (70.38 and 64.72 and P < 0.001). Besides, the results reveal that the mean score for perceived self-efficacy towards healthy eating in boys was not significantly different from that of girls (43.32 and 40.97 respectively) [Table 3].
Table 3.
Mean score of HBM components in female and male students
Pearson's correlation test showed that perceived self-efficacy has a direct significant relationship with healthy eating patterns in male and female students (r = 0.427, P < 0.001 and r = 0.362, P < 0.001 respectively). In addition, a direct and significant correlation was observed among the scores of perceived benefits and healthy eating patterns in boys and girls (r = 0.355, P < 0.001 and r =.261, P < 0.001). There was no significant relationship between the scores of perceived barriers and healthy eating among male and female students, (r = -.085, P = 0.234 and r = -.027, P = 0.647 respectively). In general the results indicate a direct and significant correlation between self-efficacy and perceived benefits and healthy eating patterns in all the students (r = 0.391, P < 0.001 and r = 0.284, P <.001 respectively). Plus no significant relationship was found between the perceived barriers’ score and the healthy eating pattern in all the students surveyed [Table 4].
Table 4.
Relationship between healthy eating behavior and components of HBM in female and male students

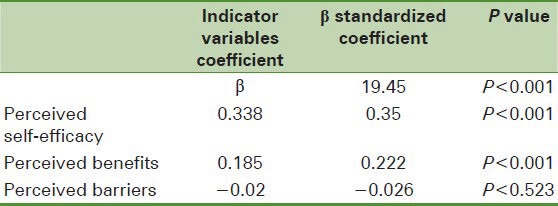
The results of the multiple linear regression analysis revealed that the most important predictive factors in the students’ healthy eating pattern score are perceived self-efficacy and perceived benefits respectively and that perceived barriers is not an influencing predictor in healthy eating patterns [Table 5].
Table 5.
Regression analysis for healthy nutrition behavior based on some components of HBM (self-efficacy, perceived benefits and perceived barriers)
DISCUSSION
The aim of this study was to determine the self-efficacy, perceived benefits of and barriers to healthy nutrition and the relationship of these variables with healthy eating patterns in the high school students of Izeh city. As the results indicate the average score for the healthy eating pattern was higher in male students compared to females. According to the popular belief shared in different societies that suggests men have less healthy eating habits compared to women,[12] there were expectations that the mean score for healthy eating in female students would exceed male students. However, the study findings did not prove that to be the case. What is certain is that eating behavior in adolescence is affected by several factors such as: Individual factors, social, physical and overall environmental factors.[13] Each of these influential factors may prevent or be an incentive for healthy nutrition in teenagers.
The results of this study also revealed that the highest mean scores for eating behavior in both gender groups was related to the eating pattern “I eat breakfast” with the mean score 3.19 in boys and 2.78 in girls. The findings also showed that 7.5% of boys and 13.7% of girls had eliminated breakfast from their diets. While in Lee and Yuen Loke's reports 55% of girls had eliminated breakfast[14] and in Erenglu's research only 49% of the subjects studied had breakfast.[15] A possible reason as to why in our research there are gender differences in eating breakfast can be the season the samples were selected. Since at the time of filling the questionnaires, the male high school students of Izeh city had afternoon classes while the females had morning classes, they probably had more time to eat breakfast alongside their families compared to the females. Based on the other findings of this study, the lowest mean score of eating behavior in both genders was related to the eating behavior “Choosing a diet with low fat and cholesterol” with a mean score of 1.85 in boys and 1.94 in girls. Given that eating behavior in adolescence is affected by several factors, it is logical to consider these factors in interventions used to improve their eating behavior. These factors include self-efficacy, perceived benefits and perceived barriers.
For this purpose, the findings of this study showed that the mean score for perceived benefits of healthy eating in females was significantly higher than male students and that there is a positive and meaningful association between the perceived benefits of the subjects surveyed and their healthy diet. A study by Steptoe and Colleagues in London in 1993 demonstrated a positive and significant correlation between the perceived benefits and the consumption of fruits and vegetables in the subjects surveyed.[16] The perceived benefits of healthy eating in different studies include: Improved cognitive and physical performance, fitness, endurance, psychological benefits, feeling good physically, and energy production,[10] improved quality of school foods and developing the norm of healthy nutrition,[17] disease prevention[18] and taking care of one's body.[19] The findings of the current study also showed that the perceived benefits of healthy eating in male students in order of importance include: Having a better feeling, being healthy, reducing the risks of cardiovascular diseases, having a more attractive physical appearance, being fit, producing more energy, reducing the risks of developing breast cancer, reducing weight, and reducing the risks of developing colon cancer while in female students benefits like: Feeling better, fitness, producing more energy, having a more attractive physical appearance, reducing the chances of cardiovascular disease, losing weight, being healthy, decreasing the risks of developing breast cancer and reducing the chances of colon cancer were stated from most important to least respectively.
The findings related to identifying the barriers to healthy eating patterns in students illustrated that there is no significant difference in the mean score for perceived barriers to healthy eating between the two genders. However, the importance of barriers is different in males and females in a way that the findings of this study revealed that the maximum mean score for barriers in boys (2.58) was dedicated to the option “because of the influence of friends and family, eating healthy is difficult for us” and in girls (2.53) to “eating outside limits my choices”. The lowest mean score for barriers to healthy eating in both genders (2.22 in girls and 2.23 in boys) was given to the option “healthy diets are not appetizing”. The other barriers to healthy eating in male students found in this study in the order of importance were: Health experts changing their guidelines, limited choices, difficulty of eating healthy food, giving up eating favorite foods, expensive costs, consuming too much time when shopping and preparing healthy foods and in female students: Expensive costs, health experts changing their guidelines, difficulties of healthy eating due to the influence of friends and family, giving up eating favorite foods, difficulty of healthy eating, and consuming too much time when shopping for healthy foods and preparing them. In other studies, having a dislike for healthy foods,[20] social factors, convenience and taste,[10] lack of time, limited access to healthy foods in schools and the lack of public concern for the absence of healthy eating recommendations,[21] the unavailability of healthy food, families choosing inappropriate diets and the belief that healthy eating is less among men,[17] effort, lack of knowledge and information, psychological and social factors, environmental factors and accessibility[22] were identified as the perceived barriers to eating healthy foods. Based on the correlation test, this study did not specify a significant inverse relationship between the perceived barriers and healthy eating patterns in students. While the study by Steptoe and colleagues in 2003 showed a significant negative relationship between perceived barriers and the intake of fruits and vegetables.[16] Another study in St. Paul showed that there is a significant negative correlation between the barriers perceived by students and the consumption of vegetables and fruits.[23] According to the other findings in this study, although there was no significant difference between the mean score for perceived self-efficacy in healthy eating in both genders there was a positive and significant correlation between perceived self-efficacy and healthy nutrition in the students surveyed. Steptoe reported that there was association between high self-efficacy and the high consumption of fruits and vegetables in low-income families in London.[16] Hossein Nejad and colleagues in their study entitled “The Role of self-efficacy in predicting eating behaviors among female students” indicated a significant and positive correlation between the mean score for dietary behavior and self-efficacy.[24] In the study by Landis and colleagues the correlation coefficient between self-efficacy and the consumption of calcium-containing foods in girls was reported to be 0.269 (P = 0.01).[25] The findings of the study by Sztainer and Croll also demonstrated that there is a significant and positive correlation between the students’ self-efficacy and their consumption of fruits and vegetables. Besides, there is a significant negative relationship between self-efficacy for healthy eating and perceived barriers to consuming fruits and vegetables.[23]
All in all, the findings of this study indicate that the role of some factors such as perceived benefits, barriers and self-efficacy in predicting healthy eating behaviors in male and female students is different, thus considering these variables and their role differences in the two genders is necessary in designing interventional programs.
CONCLUSION
The research findings indicate the predictive role of self-efficacy and perceived benefits on bettering health-related behaviors such as healthy eating. Thus, healthcare providers and experts can design health-promoting educational programs to increase self-efficacy and the understanding of healthy nutritional benefits and subsequently change not only student behavior, but the behavior of all the people in the society. Education officials can help improve students’ health-related behaviors by means of supporting adolescents, providing them with appropriate educational programs, providing them with appropriate models to improve their self-confidence to overcome obstacles and designing a comprehensive school health education curriculum that includes material relevant to the interests of healthy behavior like healthy eating.
The results of this research determined that many factors influence students’ dietary patterns and of course the role of these factors is not identical in both males and females. Given that a clear understanding of self-efficacy and the benefits of a healthy diet can help students adopt healthy eating habits, the country's health authorities should consider these factors in any future programming.
Furthermore, all the participants in this study were students studying in the 10 high schools of Izeh City and there lies this possibility that they differ from the other adolescents around the country in terms of various factors such as their socioeconomic status; therefore, it is impossible to generalize the findings of this study to all other students from different cities around Iran and this can be cited as one of the limitations of this study.
ACKNOWLEDGMENTS
Hereby the authors would like to thank the Research Department of Isfahan University of Medical Sciences that funded this study as a Master's thesis research project under the contract number 391017. The authors also wish to thank the school administrators and students who participated in this study.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Imanipoor M, Basampoor Sh, Haghani HR. Preventive behaviors of heart disease and its relationship with awareness of risk factors. Journal of Nursing and Midwifery School, Tehran University of Medicat Sciences (Hayat) 2008;14:41–9. [Google Scholar]
- 2.Imanipoor M, Haghani H. Evaluation of culturals knowledge and practice in the prevention of cardiovascular disease and some related factors. J Nurs Midwifery Shahid Beheshti Univ Med Sci. 2008;18(60):36–44. [Google Scholar]
- 3.Bahonar A, Shahnam M, Asadi-Lari M, Bashtam M, Gharipoor M, Taghdisi MH, et al. Risk factors of cardiovascular diseases among workers in Isfahan. Iran Occup Health J. 2010;7:4–10. [Google Scholar]
- 4.World Health Organization; [Last accessed 2012 Mar 14]. World Health Organization. Unhealthy diets & Physical inactivity 2009. Available from: http://www.who.int/nmh/publications/fact sheet_diet_en.pdf . [Google Scholar]
- 5.Ramezani-Tehrani F, Farahmand M, Amiri P, Paikari N, Azizi F. Women's perception regarding to healthy nutrition inhibitors: A qualitative research in Tehran lipid and glucose study (TLGS) Iran J Endocrinol Metab. 2011;13:48–57. [Google Scholar]
- 6.Mirmiran P, Bahadoran Z, Azizi F. Longitudinal study of diet quality in children and adolescents, based on the preventive recommendations for cardiovascular disease: Tehran lipid and glucose study. Iran J Endocrinol Metab. 2011;12:603–8. [Google Scholar]
- 7.Najmabadi Sh, Nojoomi M, Moradilakeh M. Composition of daily dietary fat intake in university student s’ diet. Hakim Res J. 2008;11:47–53. [Google Scholar]
- 8.Najmabadi S, Nojomi M. Evaluation of micronutrient intakes (vitamins and minerals) in university students. Med Sci J Islamic Azad Univ. 2005;15:191–6. [Google Scholar]
- 9.Motlagh ME, Ardalan G, Gheiratmand R, Majdzadeh R, Heidarzadeh A. Ratinal, methods and first results of the Iranian national programme for prevention of chronic diseases from childhood: CASPIAN study. East Mediterr Health J. 2009;15:302–14. [PubMed] [Google Scholar]
- 10.O’Dea JA. Why do kids eat healthful food? Perceived benefits of and barriers to healthful eating and physical activity among children and adolescents. J Am Diet Assoc. 2003;103:497–501. doi: 10.1053/jada.2003.50064. [DOI] [PubMed] [Google Scholar]
- 11.Reddan J, Wahlstrom K, Reicks M. Children's perceived benefits and barriers in relation to eating breakfast in schools with or without universal school breakfast. J Nutr Educ Behav. 2002;34:47–52. doi: 10.1016/s1499-4046(06)60226-1. [DOI] [PubMed] [Google Scholar]
- 12.Walker SN, Sechrist KR, Pender NJ. The health-promoting lifestyle profile: Development and psychometric characteristics. Nurs Res. 1987;36:76–80. [PubMed] [Google Scholar]
- 13.Neumark-Sztainer D, Story M, Perry CL, Casey MA. Factors influencing food choices of adolescents. J Am Diet Assoc. 1999;99:929–36. doi: 10.1016/S0002-8223(99)00222-9. [DOI] [PubMed] [Google Scholar]
- 14.Lee TR, Yuen Loke TA. Health-promoting behaviors and psychosocial well-being of university students in Hong Kong. Public Health Nurs. 2005;22:209–20. doi: 10.1111/j.0737-1209.2005.220304.x. [DOI] [PubMed] [Google Scholar]
- 15.Erenglu N, Ayranci U, Son O. Eating habits reported by secondary school students in a city of west Turkey. Eat Behav. 2006;7:348–54. doi: 10.1016/j.eatbeh.2005.11.009. [DOI] [PubMed] [Google Scholar]
- 16.Steptoe A, Porras LP, McKay C, Rink E, Hilton S, Cappuccio FP. Psychological factors associated with fruit and vegetable intake and with biomarkers in adults from a low-income neighborhood. Health Psychol. 2003;22:148–55. [PubMed] [Google Scholar]
- 17.Rojas RM, Garita C, Sanchez M, Munoz L. Barriers to and motivators for healthful eating as perceived by rural and urban costa rican adolescents. J Nutr Educ Behav. 2005;37:33–40. doi: 10.1016/s1499-4046(06)60257-1. [DOI] [PubMed] [Google Scholar]
- 18.Lopez A, Martinez GM, Kearney J, Gibney M, Martínez JA. Perceived barriers of, and benefits to, healthy eating reported by a Spanish national sample. Public Health Nutr. 1999;2:209–15. doi: 10.1017/s1368980099000269. [DOI] [PubMed] [Google Scholar]
- 19.Pawlak R, Colby S. Benefits, barriers, self-efficacy and knowledge regarding healthy foods; perception of African Americans living in eastern North Carolina. Nutr Res Pract. 2009;3:56–63. doi: 10.4162/nrp.2009.3.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jacobson JC, Finkle J, Ammerman A, Wegner S, Skinner AC, Benjamin JT, et al. Use of a tool to determine perceived barriers to children's healthy eating and physical activity and relationships to health behaviors. J Pediatr Nurs. 2011;26:404–15. doi: 10.1016/j.pedn.2010.10.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Croll J, Neumark-Sztainer D, Story M. Healthy Eating: What does it mean to adolescents? J Nutr Educ. 2001;33:193–8. doi: 10.1016/s1499-4046(06)60031-6. [DOI] [PubMed] [Google Scholar]
- 22.Maclellan DL, Gottschall PK, Larsen R. Fruit and vegetable consumption: Benefits and barriers. Can J Diet Pract Res. 2004;65:101–5. doi: 10.3148/65.3.2004.101. [DOI] [PubMed] [Google Scholar]
- 23.Bruening M, Kubik MY, Kenyon D, Davey C, Story M. Perceived barriers mediate the association between self-efficacy and fruit and vegetable consumption among students attending alternative high schools. J Am Diet Assoc. 2010;110:1542–6. doi: 10.1016/j.jada.2010.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hosein-Nejad M, Aziz-zadeh-Frozi M, Mohammad-Alizadeh S, Haghdoost AA. Role of self efficacy predictors in nutritional behaviors of Kerman high school female students in 2006-2007 academic year. J Shaeed Sdoughi Univ Med Sci, Yaz. 2007;16:49–56. [Google Scholar]
- 25.Landis C, Burant CH, Drotar D, Morgan L, Trapl E, Kwoh K. Social support knowledge and self-efficacy as correlates of osteoporosis preventive behaviors among preadolescent females. J Pediatr Psychol. 2003;28:333–45. doi: 10.1093/jpepsy/jsg023. [DOI] [PubMed] [Google Scholar]