

Abstract
The term “progestagens” covers a group of molecules including both the natural female sex hormones Progesterone and 17-hydroxy Progesterone as well as several synthetic forms, all displaying the ability to bind Progesterone receptors.
Several studies have used Progesterone and related steroids in the attempt to prevent spontaneous miscarriage, and treat recurrent miscarriage.
The present paper aims to provide a comprehensive review of the literature on progestagens effects during early pregnancy. We looked only at the results from randomized controlled trials. We found and analyzed 15 trials on the prevention of recurrent miscarriage and 2 trials on the treatment of miscarriage. The results demonstrated that there is no evidence to support the routine use of progestagens for the treatment of threatened miscarriage.
Keywords: Miscarriage, progestagens, Progesterone, 17 α OH Progesterone, 17 α OH Progesterone Caproate, recurrent miscarriage
Introduction
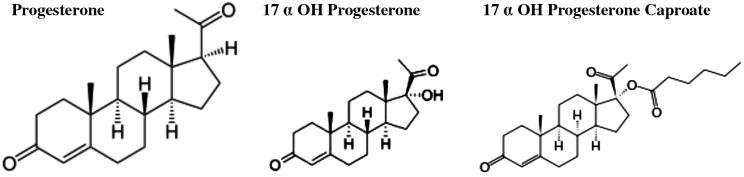
Progesterone (Fig. 1) is a steroid hormone which plays a crucial role in each step of human pregnancy.
Fig. 1. Progesterone and Progestagens.
In early pregnancy Progesterone is produced by the corpus luteum whose duration has been estimated 12 ± 2 days. This organ is fundamental for pregnancy maintenance until the placenta (syncytiotrophoblast) takes over its function at 7-9th week of gestation, just after the expression of major histocompatiblity complex antigens is suppressed in extra-embryonic fetal tissue.
Progesterone is an essential hormone in the process of reproduction. Indeed, it induces secretory changes in the lining of the uterus and is essential for a successful implantation of the embryo. Moreover, Progesterone modulates the immune response of the mother to prevent rejection of the embryo, and enhances uterine quiescence and suppresses uterine contractions. Therefore it is theoretically plausible that P supplementation may reduce the risk of miscarriage in women with a history of recurrent miscarriages. Several studies have used Progesterone and related steroids (progestagens- Fig. 1) in the attempt to prevent spontaneous miscarriage and to increase the embryo implantation rates in assisted reproduction programmes. The term “progestagens” cover a group of molecules including both the natural female sex hormones Progesterone and 17-hydroxy Progesterone (17P) as well as several synthetic forms, all displaying the ability to bind Progesterone receptors.
Although pharmacokinetics and pharmacodynamics features of progestagens have been studied, their use in human pregnancy remains controversial, i.e. the way of administration. Indeed, progestagens could be administered by three routes: orally, vaginally or intramuscularly. Oral administration guarantees optimal compliance by patients but shows many disadvantages; this route also results in side effects such as nausea, headache and sleepiness. The vaginal route results in higher concentrations in the uterus but does not reach high and constant blood levels. The drug administered intramuscularly occasionally induces non-septic abscesses, although it is the only route which results in optimal blood levels (Whitehead et al., 1990; Szabo and Szilagyi, 1996; Cunningham, 2001; Di Renzo et al., 2005; Christian et al., 2007). Several reports hypothesized an association between intrauterine exposure to progestagens in the first trimester of pregnancy and genital abnormalities in male and female fetuses. This was due to the possible up-regulation of androgen receptor operated by pharmacological doses of these steroids. However, maternal safety of progestagens has been reported in different trials. Neonatal safety has been evaluated in only one trial where mothers have been treated with 17 Progesterone. No effects of general health status, external genitalia, and psychomotor development have been reported at follow-up. Since the paucity of data, ongoing trials are encouraged to include the follow-up of neonates in their study design (Mosby, 2001).
The present paper aims to provide a comprehensive view of the literature on the effects of progestagens during early pregnancy. We describe the effects of progestagens for preventing recurrent miscarriages and managing threatened miscarriage.
Miscarriage is defined as pregnancy loss before 23 weeks’ gestation, based on the first day of the last menstrual period. Miscarriage is associated with considerable physical and psychological morbidity, particularly in developing countries (World Health Organization, 1992). Haemorrhage into the decidua basalis and necrotic changes in the tissues adjacent to the bleeding usually accompany abortion; the ovum becomes detached and stimulates uterine contractions that result in expulsion (Cunningham, 2001).
Recurrent miscarriage has been defined as 3 or more consecutive episodes of spontaneous pregnancy losses with the same biological father (World Health Organization, 1992). Extensive investigation of women involved will fail to find a recognisable cause in up to half of the cases. Luteal phase defects, immunotolerance derangements, chromosomal anomalies and endocrine disorders are the most common recognisable causes. Accepting an independent risk of miscarriage to be 15%, a second loss could be calculated to occur at a rate of 2-3% while a third loss is expected in 0.34% of women.
More than 80% of miscarriages occur before the 12th week, and the rate decreases rapidly thereafter. It is a common complication of pregnancy occurring in 15% to 20% of all clinically recognized pregnancies with 1% to 2% of couples suffering a recurrent early loss. It is thought, however, that the true incidence of early spontaneous miscarriage may be much higher. Indeed, after implementation of assisted reproduction techniques we are able to detect biochemical pregnancies and therefore to conclude that the rate of early spontaneous miscarriage in the first trimester is higher than expected (Everett, 1997).
Chromosomal anomalies cause at least half of these early miscarriages. The risk increases with parity and at the extremes of maternal age (>34 years and <20 years old). Other risk factors for miscarriage include maternal infections (such as vaginitis, urinary tract infections), endocrine abnormalities (diabetes mellitus, hypothyroidism, pituitary adenoma), insufficient production of Progesterone by the corpus luteum (short and/or abnormal luteal phase), polycystic ovary syndrome, drug use, environmental factors, maternal autoimmune disorders (such as anti-phospholipids antibodies), previous history of two or more miscarriages and acquired or inherited uterine malformations (Szabo and Szilagyi, 1996). Despite all the above recognised or supposed factors, the cause of miscarriage cannot be identified in almost 50% of cases. Threatened miscarriage manifests itself through vaginal bleeding, with or without abdominal pain, while the cervix is closed and the fetus is viable inside the uterine cavity. The introduction of ultrasound scans in the management of bleeding in early pregnancy has improved the diagnosis tremendously (Hemminki, 1998).
During the past 50 years several trials investigated the use of progestagens for the prevention of miscarriage. Actually the therapeutic value of progestagens remains to be established. This might be due to the poor design of the studies which evaluated hormone effectiveness. Moreover, a lot of different aetiologies are associated with threatened miscarriages and heterogeneity of studies has not been accounted for.
Methods
Literature searches were performed in The Cochrane Library, only randomized controlled trials (RCTs) were considered. The search terms were as follows: “progestagens”, “miscarriage”, “recurrent miscarriage”. We performed a search about all types of progestagens, their applications and potential effects for preventing recurrent miscarriage and for managing miscarriage, regardless of the dose, duration or route of administration compared with placebo, no treatment or other intervention.
All sources of information were read and evaluated by one of the authors (GD), and were later independentely checked by another author (VV).
Results
Two recent Cochrane Reviews (Haas and Ramsey, 2009; Wahabi et al., 2011) selected the randomized controlled trials (RCT) or quasi-randomized controlled trials published between 1966 and 2006. They included all types of progestagens in the prevention of miscarriage (Haas and Ramsey, 2009) and for the treatment of threatened miscarriage (Wahabi et al., 2011), regardless of the dose, duration or route of administration and compared with placebo, no treatment or other interventions. No further RCTs were published after those included in the Cochrane Review.
Wahabi et al. (2011) selected the trials published in 7 databases and references from relevant articles. The authors included only the trials where the administration of progestagens started before pregnancy and continued during pregnancy. Twenty-nine studies were potentially eligible for inclusion, of these, 15 studies were included after applying the inclusion criteria. The characteristics of these RCTs are described in Table 1.
Table I. Characteristics of randomized controlled trials analized for preventing recurrent miscarriage (RCT: Randomized Controlled Trial, PTB: preterm birth).
| Authors/year | Population studied | Intervention | Comparison | Outcome measured |
| El Zibdeh et al. 2005 | Pregnant women (aged <35 years) with at least 3 consecutive unexplained abortions with same partner | - Dihydrogesterone | RCT vs no treatment | Miscarriage, PTB, fetal malformations |
| - Oral | ||||
| - Until miscarriage or 12 weeks | ||||
| - N = 180/180 | - 10 mg twice daily | |||
| Goldzieher et al.1964 | Women who never had a term pregnancy and with a history of 2 or more miscarriages or with a history of 1 or more term pregnancy followed by a minimum number of 2 consecutive miscarriages | - Medroxy Progesterone acetate | Double blind, RCT vs placebo | Miscarriage, PTB |
| - Oral | ||||
| - Not stated | ||||
| N = 54/54 | - 10 mg daily | |||
| Klopper et al. 1965 | Women who had 2 or more miscarriages, no pregnancy beyond 28 weeks’ gestation, were less than 10 weeks into the current pregnancy and with no other obvious causes of miscarriage | - Cyclopentyl onol ether of Progesterone | Double blind, RCT vs placebo | Miscarriage |
| - Oral | ||||
| - Not stated | ||||
| - 50 mg twice daily | ||||
| Moller et al. 1965 | Women with a positive pregnancy test. | - Medroxy Progesterone acetate | Double blind, RCT vs placebo | Miscarriage |
| - Oral | ||||
| N = 40/40 | - 20 mg/day for 3 days, followed by 10 mg/day for 11 days | |||
| Moller et al. 1965 | Women with a positive pregnancy test. | - Medroxy Progesterone acetate | Double blind, RCT vs placebo | Miscarriage |
| - Oral | ||||
| N = 63/63 | - 40 mg/day for 3 days, followed by 20 mg/day for 11 days | |||
| Moller et al. 1965 | Women with a positive pregnancy test. | - Medroxy Progesterone acetate | Double blind, RCT vs placebo | Miscarriage |
| - Oral | ||||
| N = 153/153 | - 80 mg/day for 3 days, followed by 40 mg/day for 11 days | |||
| Levine et al. 1964 | Women with 3 consecutive miscarriages of less than 16 weeks’ gestation and with no signs of threatened miscarriage in the current pregnancy | - 17OHPc | Double blind, RCT vs placebo | Miscarriage, PTB |
| - IM | ||||
| - until miscarriage or 36th week | ||||
| N = 56/30 | - 500 mg weekly | |||
| Anderson et al. 2002 | Women having undergone IVF or ICSI with a positive pregnancy test 14 days after transfer | - Progesterone vaginally | RCT vs no treatment | Miscarriage |
| - 3 weeks | ||||
| N = 303/303 | - 200 mg 3 times daily | |||
| Reijnders et al. 1988 | One or more of the following criteria: pregnancy after ovulation induction; 2 or more previous miscarriages; period of infertility for more than 12 months. Evidence of a viable fetus at 6 weeks of pregnancy | - 17OHPc | Double blind, RCT vs placebo | Miscarriage, PTB |
| - i.m. | ||||
| - from 7th to 12th week | ||||
| N = 64/64 | - 500 mg/week | |||
| Shearman et al. 1963 | Women with 2 or more consecutive abortions and low or falling pregnanediol levels | - 17OHPc | Double blind, RCT vs placebo | Miscarriage |
| - i.m. | ||||
| N = 50/50 | - Up to 8th week 250 mg/ weekly; then increasing dose to 500 mg till 16th week; then reducing doses to 250 mg/weekly until 24th week | |||
| Berle et al. 1980 | Women up to 20 weeks gestation with bleeding | - 90% received oral allylestrenol 15-20 mg/day | Double blind, RCT vs placebo | Miscarriage |
| - 10% received 250 mg of i.m. 17OHPc daily or every 2 days | ||||
| N° = 300/300 | - Duration not stated | |||
| Tognoni et al. 1980 | Women with threatened miscarriage up to 14 weeks’ gestation | - Oral allylestrenol 10 mg/d | RCT vs placebo | Miscarriage |
| - 25 mg 17HP im every 5 d | ||||
| N° =145/139 | - 8 weeks | |||
| Gerhard et al. 1987 | Women with vaginal bleeding in pregnancy and a closed cervical os | - Progesterone | Double blind, RCT vs placebo | Miscarriage, birth weight, preterm labour |
| - Vaginal suppositories | ||||
| N° = 64/35 | - 25 mg twice/day | |||
| Swyer & Daley 1953 | Women with 2 or more consecutive miscarriages before 12 weeks’ gestation | - 6 × 25 mg Progesterone pellets inserted in the gluteal muscle | RCT vs control group | Miscarriage, birth weight, PTB, stillbirth |
| N = 113/113 | ||||
| Corrado et al. 2002 | Women undergoing mid-second trimester amniocentesis | - Progesterone IM. 200 mg/day for 3 days followed by 17OHPc IM 340 mg twice/week | RCT vs control group | Miscarriage, birth weight, preterm delivery |
| N = 616/584 | - Duration unclear |
Haas and Ramsey (2009) selected the RCTs or quasi-randomized controlled trials that appeared in 30 journals and the proceedings of major conferences describing all types of progestagens in the treatment of threatened miscarriage. Participants were all pregnant women, with a history of threatened miscarriage and a confirmed viable pregnancy. Thirty-four studies were potentially eligible for inclusion. Only 2 were included after applying the inclusion criteria (Gerhard et al., 1987; Palagiano et al., 2004). The characteristics of these RCTs are described in TTable 2.
Table II. Characteristics of included studies for treating miscariages.
| Authors/year | Population studied | Intervention | Comparison | Outcomes measured |
| Gerhard et al. 1987 | Women in the first trimester of pregnancy with confirmation of fetal viability by ultrasound scan | Progesterone | Double blind, RCT vs placebo | Miscarriage, birth-weight, preterm labour |
| - Vaginal suppositories | ||||
| - 14 days after bleeding stopped | ||||
| N = 64/35. | - 25 mg twice/day | |||
| Palagiano et al. 2004 | 50 women with previous diagnosis of inadequate luteal phase, threatened miscarriage and confirmed fetal viability | Progesterone | RCT vs placebo | Pain relief uterine contractions, blood loss |
| - Vaginal suppositories | ||||
| - 5 days | ||||
| - 90 mg/day |
These two trials met the inclusion criteria and involved 85 participants. Due to a paucity of data, subgroup analysis for early and late miscarriage, effect of progestagens by type, dose, and route of administration could not be carried out.
Discussion
The overall meta-analysis conducted on the use of progestagens for the treatment of recurrent miscarriages (Haas and Ramsey, 2009) showed no statistically significant difference in miscarriage rates between progestagens and placebo groups (Peto OR 0.98; 95% CI 0.78 -1.24). The analysis regarding the method of administration also showed no statistically significant difference between progestagens and placebo groups.
No evidence for an effect favouring the use of progestagens in women with recurrent miscarriage was found when compared to placebo (Peto OR 1.11, 95% CI 0.79-1.56, P = 0.54). Four studies (Shearman and Garrett, 1963; Levine, 1964; Reijnders et al., 1998; Corrado et al., 2002) compared intramuscular progestagens with placebo, the results showed no differences in miscarriages between the two groups (Peto OR 0.77; 95% CI 0.36-1.68, P = 0.52). Only one study compared vaginally administered progestagens with placebo, a second one comparing it with no treatment. The incidence of recurrent miscarriage was similar in both groups (Peto OR 0.74; 95% CI0.40-1.35, P = 0.32).
The analysis concerning recurrent miscarriage considered 4 trials, of these 2 trials (Levine, 1964; El-Zibdeh, 2005) enrolled only women who had suffered three or more miscarriages, 2 others (Swyer and Daley, 1953; Goldzieher, 1964) provided separate pregnancy outcome data by number of previous consecutive pregnancy losses. The results showed a reduction in miscarriage in favour of those in the progestagens group (Peto OR 0.38; 95% CI 0.20 to 0.70, P = 0.002). This finding however should be approached with caution as numbers are small.
Meta-analysis of the effect of vaginal Progesterone on miscarriage when compared to placebo (Wahabi et al., 2011) showed a point estimate which suggests a reduction of miscarriage rate with the use of Progesterone (risk ratio 0.47; 95% confidence interval 0.17 to 1.30), but the uncertainty about the outcome of this study is due to the small sample size.
Conclusion
Based on scarce data there is no evidence to support the routine use of progestagens for the treatment of threatened miscarriage. Information about potential harms to the mother or child, or both, with the use of progestagens is lacking. There has been much speculation about progestagens but the results of these meta-analysis show no statistically significant difference between women receiving progestagens for preventing threatened miscarriage or miscarriage when compared to placebo, other treatments or no treatment. Further, larger RCTs investigating potential harms as well as benefits, are urgently needed. A finding of a significantly reduced miscarriage rate in women with a history of recurrent miscarriage was found only in studies that included women with at least three miscarriages. This finding was obtained with different types of progestagens and therefore deserves further study before entering in clinical practice.
References
- Anderson NA, Todorovic B, Schmidt K, et al. Progesterone supplement during early gestations after IVF or ICSI has no effect on the delivery rates: a randomized controlled trial. Hum Reprod. 2002;17:357–361. doi: 10.1093/humrep/17.2.357. [DOI] [PubMed] [Google Scholar]
- Berle P, Budenz M, Michaelis J. Is hormonal therapy still justified in imminent abortion? Z Geburtshilfe Perinatol . 1980;184:353–358. [PubMed] [Google Scholar]
- Christian MS, Brent RL, Calda P. Embryo-fetal toxicity signals for 17alpha-hydroxyprogesterone caproate in high-risk pregnancies: a review of the non-clinical literature for embryo-fetal toxicity with progestins. J Matern Fetal Neonatal Med. 2007;20:89–112. doi: 10.1080/14767050601178758. [DOI] [PubMed] [Google Scholar]
- Corrado F, Dugo C, Cannata M, et al. A randomised trial of progesterone prophylaxis after midtrimester amniocentesis. Eur J Obstet Gynecol Reprod Biol. 2002;100:196–198. doi: 10.1016/s0301-2115(01)00418-3. [DOI] [PubMed] [Google Scholar]
- Cunningham FG. Williams obstetrics. Section IX. 21st Edition. McGraw-Hill: 2001. Reproductive success and failure. [Google Scholar]
- Di Renzo GC, Mattei A, Gojnic M, et al. Progesterone and Pregnancy. Current opinion. Obstet Gynecol. 2005;17:598–600. doi: 10.1097/01.gco.0000191899.84567.4d. [DOI] [PubMed] [Google Scholar]
- Zibdeh MY. J Steroid Biochem Mol Biol. 2005;97:431–434. doi: 10.1016/j.jsbmb.2005.08.007. [DOI] [PubMed] [Google Scholar]
- Everett C. Incident and outcome of bleeding before the 20th week of pregnancy: prospective study from general practice. . BMJ. 1997;315:32–34. doi: 10.1136/bmj.315.7099.32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gerhard I, Gwinner B, Kruse W, et al. Biol Res in Pregnancy Perinatol. 1987;8:26–34. [PubMed] [Google Scholar]
- Goldzieher JW. Double-blind trial of a progestin in habitual abortion. JAMA. 1964;188:651–654. doi: 10.1001/jama.1964.03060330031008. [DOI] [PubMed] [Google Scholar]
- Haas DM, Ramsey PS. Progestogen for preventing miscarriage. Cochrane Database Syst Rev. 2009;(CD003511) doi: 10.1002/14651858.CD003511.pub2. [DOI] [PubMed] [Google Scholar]
- Hemminki E. Treatment of miscarriage: current practice and rationale. Obstet Gynecol. 1998;91:247–253. doi: 10.1016/s0029-7844(97)00606-6. [DOI] [PubMed] [Google Scholar]
- Klopper A, MacNaughton M. Hormones in recurrent abortion. J Obstet Gynaecol Br Commonw. 1965;72:1022–1028. [Google Scholar]
- Levine L. Habitual abortion. A controlled clinical study of progestational therapy. West J Surg Obstet Gynecol. 1964;72:30–36. [PubMed] [Google Scholar]
- Moller K, Fuchs F. Double blind controlled trial of 6- methyl-17-acetoxyprogesterone in threatened abortion. J Obstet Gynaecol Br Commonw. 1965;72:1042–1044. [Google Scholar]
- Mosby Incorporated. Medroxyprogesterone acetate. Harcourt Health Sciences Incorporated. 2001 [Google Scholar]
- Palagiano A, Bulletti C, Pace MC, et al. Effects of vaginal progesterone on pain and uterine contractility in patients with threatened abortion before twelve weeks of pregnancy. Ann N Y Acad Sci. 2004;1034:200–210. doi: 10.1196/annals.1335.022. [DOI] [PubMed] [Google Scholar]
- Reijnders FJL, Thomas CMG, Doesburg WH, et al. Endocrine effects of 17 alphahydroxyprogesterone caproate during early pregnancy: a double-blind clinical trial. Br J Obstet Gynaecol. 1988;95 doi: 10.1111/j.1471-0528.1988.tb12797.x. [DOI] [PubMed] [Google Scholar]
- Shearman R, Garrett W. Double-blind study of effect of 17-hydroxyprogesterone caproate on abortion rate. BMJ. 1963;1:292–295. doi: 10.1136/bmj.1.5326.292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swyer GIM, Daley D. Progesterone implantation in habitual abortion. BMJ. 1953;1:1073–1086. doi: 10.1136/bmj.1.4819.1073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szabo I, Szilagyi A. Management of threatened abortion. Early Pregnancy. 1996;2:233–240. [PubMed] [Google Scholar]
- Tognoni G, Ferrario L, Inzalaco M. Progestogens in threatened abortion. Lancet. 1980;2:1242–1243. doi: 10.1016/s0140-6736(80)92496-4. [DOI] [PubMed] [Google Scholar]
- Wahabi HA, Abed Althagafi NF, Elawad M, Al Zeidan RA. Progestogen for treating threatened miscarriage. Cochrane Database Syst Rev. 2011;(CD005943) doi: 10.1002/14651858.CD005943.pub4. [DOI] [PubMed] [Google Scholar]
- Whitehead MI, Hillard TC, Crook D. The role and use of progestogens. 1990;75:59S–76S. [PubMed] [Google Scholar]
- World health Organization. Vol. 1. Geneva: 1992. International Statistical Classification of Diseases and Related Health Problems, 10th Edition. [Google Scholar]