

Abstract
Objective
The objective of this study is to determine the normal value of 3D left ventricular (LV) twist in subendocardial, mid-wall and subepicardial layers, as well as to study the effects of aging on 3D LV twist by tagged MR motion tracking techniques. Three dimensional motion detection based on 3D tagged MR images is robust to out-of-plane motion error; while 2D motion detection is inherently unable to analyze the 3D cardiac motion and may lead to inaccurate results.
Methods
The 3D LV volumetric images were acquired in 52 normal adult subjects (aged 21-82) and were analyzed by using 3D HARmonic phase (HARP) technique. HARP technique provided the 3D displacement fields and the displacements were utilized to compute the rotational values. LV twist was defined as apical rotation relative to the basal rotation, in the 3D coordinates. The LV twist values of subendocardial, mid-wall and subepicardial layers were analyzed separately. The measured parameters in this study were: peak apical rotation, peak basal rotation, and peak LV twist.
Result
Looking at the apex, the normal LV maintains a clockwise rotation in the LV basal plane and a counterclockwise rotation in the LV apical plane. In general, the apical and basal rotation values increase during the aging process, leading to an increased value of LV twist. Peak epicardial LV twist is (10.4±2.6 degrees) which is lower than the mid-wall LV twist (11.3±2.2 degrees) and endocardial LV twist (12.1±2.6 degrees) in the young group (21-35 years old). Also, peak epicardial LV twist is (12.2±2.6 degrees) which is lower than the mid-wall LV twist (14.4±2.8 degrees) and endocardial LV twist (14.7±2.5 degrees) in the middle aged group (21-35 years old). In a similar way, peak epicardial LV twist is (14.8±2.9 degrees) which is lower than the mid-wall LV twist (15.7±3.6 degrees) and endocardial LV twist (16.7±3.0 degrees) in the old group (50-65 years old). Regarding the older group (more than 65 years old), peak epicardial LV twist is (15.9±3.1 degrees) which is lower than the mid-wall LV twist (16.2±3.4 degrees) and endocardial LV twist (18.3±3.0 degrees).
Conclusions
It is feasible to measure the subepicardial, mid-wall and subendocardial twist in tagged MR images. The twist value gradually increases in the aging process. Outside layers have greater twist values compared to the inside layers.
Keywords: Cardiac torsion, HARmonic phase (HARP), motion detection, tagged magnetic resonance imaging (MRI), twist
Introduction
The heart is composed of oblique myocardial fibers that create a wringing contraction to pump the blood into aorta. Many studies have shown a relationship between dynamic cardiac rotation and cardiac systolic (1-4) and diastolic function (5). A popular way to analyze the cardiac rotation is speckle tracking echocardiography (STE). STE is an image processing method to analyze myocardial deformation, independent of cardiac translation and insonation angle. STE is non-invasive and can be an indicator of cardiac function (6-9). However, 2D STE can only provide 2D motion vectors and suffers from out-of-plane motion error (10,11). Additionally, selection of optimal imaging planes for 2D STE is difficult due to limited acoustic windows and oblique orientation of the heart. Failure to acquire the standard plane can lead to inaccuracy in the measurements. Moreover, measuring the left ventricle (LV) twist using 2D STE needs two apical and basal slices in two different cardiac cycles, which necessitates separate breath-holds and leads to less accurate analysis. Although 3D twist analysis is feasible in echocardiography data (12), echocardiography images are inherently noisy and prone to artifacts; while magnetic resonance imaging (MRI) images can provide us with excellent anatomical resolution. Tagged MRI, in particular, is a method to embed non-invasive tag lines on the cardiac tissue and track it over the cardiac cycle. Motion detection using tagged MRI has been widely used in the literature in order to analyze the cardiac dynamics (13,14).
The heart has a wringing motion in the direction of its inter-tangled fibers. Cardiac twist is caused by the relative torsion of the heart with respect to its axis. It has been shown that the cardiac twist values change during the aging process (15,16). Although the underlying pathology for age-related twist changes is not known well, it may be, partly, due to the age related myocardial fiber changes as well as decreased calcium uptake by the sarcoplasmic reticulum, resulting in prolonged myocardial relaxation (15,16).
Previously, we have studied the twist value and its relationship with age in a group of normal subject using 3D echocardiography (17). Tagged MRI is used in this study to accurately measure the displacements using non-invasive tag lines. Since the twist value is different close to epicardium and endocardium, the results are classified for subendocardium, mid-wall and sub-epicardium.
LV twist analysis can provide the clinicians with valuable indices. Twist values can differentiate two clinically similar conditions: constrictive pericarditis and restrictive cardiomyopathy. Additionally, the LV twist value decreases in LV systolic dysfunction and depressed ejection fraction, but it does not decrease in normal ejection fraction and diastolic dysfunction. Another interesting phenomena is that the apex and base of the LV rotate in the same direction during systole in patients with LV Non-compaction Cardiomyopathy (9). Since tagged MRI is known as an excellent method for cardiac motion detection, it can lead to more accurate twist measures. Moreover, unlike echocardiography, tagged MRI can acquire full LV volume in most of the subjects; while echocardiography suffers from bone-air interaction and drop-out artifacts.
This study aims to (I) measure the normal value of 3D LV twist in subepicardial, mid-wall and subendocardial layers in a large group of healthy volunteers; and (II) analyze the effect of aging on the 3D LV twist among different subjects categorized by age.
Methods
The study was approved by the local institutional review board (Tehran University of Medical Science, Tehran, Iran). Fifty two healthy, non-obese (body mass index <27 kg/m2) volunteers in the range of 21-82 years old were recruited. The subjects were free of MRI contraindications such as ferromagnetic implants, claustrophobia, arrhythmia, shrapnel, dyspnea that precluding a 10-15 s breath-hold. Inclusion and exclusion criteria are described in Table 1. An informed consent was obtained from the subjects. History taking, physical exam, electrocardiogram (ECG), 2D and 3D echocardiography studies were performed in the first step. The vital signs of the selected subjects were in the normal range. The subjects were divided into four groups based on age (Group I: 21-35 years, group II: 36-50 years, group III: 51-65 years, and group IV: >65 years). Table 2 shows the four classes, number of males and females, patient height, patient weight, end diastolic LV diameter, early diastolic peak velocity, and late diastolic peak velocity.
Table 1. Inclusion and exclusion criteria.
| Inclusion | Exclusion |
|---|---|
| Age more than 21 and less than 82 | Chronic diseases (hypertension, diabetes, chronic cardiac, lung, renal or liver disease) |
| Body mass index <27 kg/m2 | Claustrophobia |
| Ferromagnetic implants or shrapnel | |
| Arrhythmia | |
| Dyspnea precluding a 10-15 s breath-hold | |
| Any medication | |
| Abnormal EKG | |
| Structural or valvular abnormality in 2D echocardiography |
Table 2. General demographic and echocardiographic characteristics of the subjects.
| Age | Number [males, females] | Height (cm) | Weight (kg) | Heart rate (/min) | End diastolic LV length (cm) | Early diastolic peak velocity (E) (m/s) | Late diastolic peak velocity (A) (m/s) |
|---|---|---|---|---|---|---|---|
| 21-35 | 12 [5, 7] | 170.2±10.7 | 74.2±10.4 | 74±9.5 | 7.0±0.4 | 0.86±0.15 | 0.75±0.36 |
| 36-50 | 14 [7, 7] | 170.3±10.0 | 75.7±9.4 | 75±9.3 | 7.2±0.8 | 0.81±0.73 | 0.74±0.54 |
| 51-65 | 14 [6, 8] | 169.8±9.6 | 79.0±8.1 | 74±8.5 | 7.1±0.5 | 0.70±0.59 | 0.84±0.77 |
| >65 | 12 [8, 4] | 168.2±9.6 | 74.2±8.8 | 74±9.0 | 6.9±0.4 | 0.65±0.22 | 0.88±0.80 |
LV, left ventricular.
Image acquisition and processing
2D echocardiographic studies were performed with a commercially available system (iE33, Philips, Best, The Netherlands) using a S5-1 transducer. Peak early (E) and late (A) filling velocities, and E/A ratio were measured using the LV inflow pattern (measured at the tips of the mitral valve). After a comprehensive standard echocardiographic examination, 3D echocardiography series were recorded. 3D echocardiography was performed using a Philips iE 33 ultrasound machine (iE33; Philips, Best, The Netherlands) with an X3-1 matrix transducer, placed on the apical position. Width and depth of the field of view were adjusted to allow inclusion of LV walls within the imaging field of view.
Tagged MRI data acquisition was performed using 1.5T Siemens scanner, TE/TR 2/25 ms, Flip Angle 45, spatial resolution 1.0 mm × 1.0 mm, slice thickness 8 mm, and spatial size 256×256×8 pixels. Since the heart rate is different in the subjects, it is important to align the cardiac cycle timing. Spline interpolation was used to change the number of frames of cardiac cycle. To analyze the 3D motion, a previously validated algorithm was utilized by the authors (14). The endocardial and epicardial contours were delineated by experts. Two MRI technicians with more than five years of experience segmented and analyzed the data. The second operator helped to compute the inter-operator variations as will be discussed in section 2.5. The images were presented to the technicians in a graphical user interface and they independently segmented the endocardium and epicardium. The algorithm, automatically, assumes that the thickness of endocardium, midwall and epicardium is the same, in order to segment the endocardial, midwall and epicardial layers. Since tagged MR images cannot provide histological data to analyze the fiber direction, this assumption can be helpful to analyze the motion in each cardiac layer. In the next step, it is necessary to compute the basal and apical cross sections using the 3D segmented cardiac volume. The left ventricular center line was computed using the segmented endocardial surface. The most basal slice was defined as the closest image to atria showing LV myocardium around its perimeter and the most apical image was the last image with a detectable LV lumen. The basal cross section was defined as the most basal cross section perpendicular to the centerline. The apical cross section was defined as the most apical cross section perpendicular to the centerline. An expert observed the results and the motion of the 3D images to qualitatively assess the function of the algorithm. In the final step rotation was computed. Rotation is the component of the displacement that is in the direction of rotational unit vector. To compute pure rotation, inner product of the displacement and the rotational unit vector was calculated. In order to obtain the average rotation or twist values, the summation of the values of rotation or twist inside a specific region (endocardium, epicardium or mid-wall) was divided by total the number of pixels in that specific region. The twist values for endocardial, midwall and epicardiac layers are compared using correlation analysis and the results are reports as P values.
Definition of twist, and rotation
The myocardial rotation around the long axis of the LV in each short-axis plane is defined as 2D LV rotation. The difference in LV rotation between the apical and basal plane is considered as “LV twist”. Peak LV twist can be computed as (peak LV twist = peak apical rotation—peak basal rotation) (18). It is noteworthy that the direction of the rotation in apical and basal slices is usually opposite. The measured parameters in this study were: peak apical rotation, peak basal rotation, and peak twist.
Statistical analysis
The statistical analysis was performed by Matlab software (Natick, MA, USA). Quantitative twist values were presented as means ± SD. Data were analyzed using analysis of variance to compare the degree of twist and age groups. Differences between patient classes were validated by one-way analysis of variance. Categorical variables were compared by Chi-square test. The association between age and cardiac parameters were analyzed by Student t-test. Statistical differences were considered significant at P value <0.05.
Intra-operator reproducibility
Twenty volunteers were randomly selected for an additional motion detection by the same operator after four months, in order to analyze the reproducibility of the algorithm by the same user. The second set of images were segmented and analyzed by the same expert on the same cardiac cycle (one additional analysis on the same cycle). The expert was unaware of the results. Reproducibility error was measured using, where is the first measurement and is the second measurement.
Inter-operator reproducibility
In a similar process, 20 volunteers were randomly selected for an additional motion detection by another operator, who was unaware of the results. The second set of images were independently segmented and analyzed by the blind expert. The measurements were performed one time on the same cardiac cycle.
Results
The demographic and echocardiographic data of the subjects, classified based on age groups, is shown in Table 2.
Feasibility of obtaining LV motion and twist indices
LV volume cannot be captured in some patients due to motion artifact. Image quality of the LV volume was insufficient for twist analysis in 6 cases out of 58 subjects. Therefore, 52 subjects with full LV volume were left in the study that led to complete analysis of LV rotation parameters.
Cardiac motion and twist
The displacements are shown in Figure 1 for one example. The apical and basal twist curves corresponding to the endocardium, mid-wall and epicardium are shown in Figure 2. As a common standard, the LV twist is viewed from the apex. Counterclockwise rotation is considered positive, while clockwise rotation is considered negative.
Figure 1.
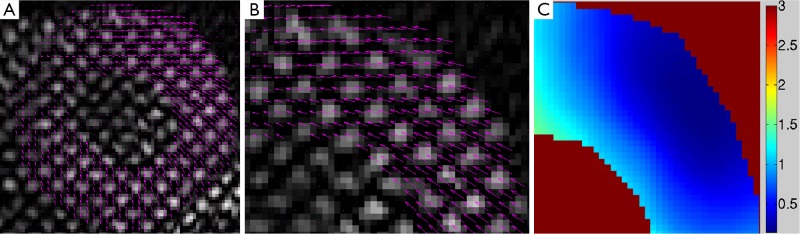
(A) Displacement vectors of one slice of tagged MR images in one subject. The magenta vectors show the twist motion of the myocardium during systole; (B) Zoomed-in view of the motion field to better show the endocardial, mid-wall and epicardial vectors; (C) Pixel-wise twist values for different cardiac layers.
Figure 2.

(A) Normal basal and apical rotational values for different age groups in the sub-epicardium; (B) normal LV twist values for different age groups in the sub-epicardium; (C) normal basal and apical rotational values for different age groups in the mid-wall; (D) normal LV twist values for different age groups in the mid-wall; (E) normal basal and apical rotational values for different age groups in the sub-endocardium; (F) normal LV twist values for different age groups in the sub-endocardium.
As shown in Table 3 and Figure 2, the Peak twist rate for 21-80 years old subjects ranges between 10-19 degrees. As expected, peak A wave velocity increases with aging, while peak E wave velocity and decreases. Peak epicardial LV twist is (10.4±2.6 degrees) which is lower than the mid-wall LV twist (11.3±2.2 degrees) and endocardial LV twist (12.1±2.6 degrees) in the young group (21-35 years old). Also, peak epicardial LV twist is (12.2±2.6 degrees) which is lower than the mid-wall LV twist (14.4±2.8 degrees) and endocardial LV twist (14.7±2.5 degrees) in the middle aged group (21-35 years old). In a similar way, peak epicardial LV twist is (14.8±2.9 degrees) which is lower than the mid-wall LV twist (15.7±3.6 degrees) and endocardial LV twist (16.7±3.0 degrees) in the old group (50-65 years old). Regarding the older group (more than 65 years old), peak epicardial LV twist is (15.9±3.1 degrees) which is lower than the mid-wall LV twist (16.2±3.4 degrees) and endocardial LV twist (18.3±3.0 degrees). The Pearson correlation analysis of peak twist value and age shows a weak but meaningful relationship (r=0.31, P<0.001). A regression analysis shows that midwall twist is close to the total twist value (r=0.97, P<0.001). Averaged epicardial twist is about 1.21 times greater than midwall twist (P<0.001) and averaged endocardial twist is about 0.82 times smaller than midwall twist based on our regression analysis (P<0.001).
Table 3. Averaged peak apical, basal and twist values in epicardium, mid-wall and endocardium of different age groups. The total twist shows the twist value for combined endocardium, mid-wall and epicardium.
| Age | Region | Peak apical rotation (degrees) | Peak basal rotation (degrees) | Peak twist (degrees) |
|---|---|---|---|---|
| 21-35 | Endocardium | 8.3±1.4 | –5.2±1.3 | 12.1±2.6 |
| Midwall | 6.9±1.6 | –4.8±1.6 | 11.3±2.2 | |
| Epicardium | 5.5±1.3 | –4.2±1.8 | 10.4±2.6 | |
| 36-50 | Endocardium | 9.4±1.8 | –7.5±1.5 | 14.7±2.5 |
| Midwall | 7.9±1.4 | –6.1±1.8 | 14.4±2.8 | |
| Epicardium | 6.3±1.3 | –5.8±1.6 | 12.2±2.6 | |
| 51-65 | Endocardium | 11.3±1.5 | –8.9±1.3 | 16.7±3.0 |
| Midwall | 9.8±1.7 | –7.4±1.8 | 15.7±3.6 | |
| Epicardium | 7.8±1.3 | –6.3±1.5 | 14.8±2.9 | |
| >65 | Endocardium | 11.8±1.8 | –9.4±1.4 | 18.3±3.0 |
| Midwall | 10.5±1.3 | –8.0±1.7 | 16.2±3.4 | |
| Epicardium | 8.4±1.7 | –6.5±1.7 | 15.9±3.1 |
The intra-operative variation for endocardium, mid-wall and epicardial layers was 2.09%±1.43%, 2.24%±1.87%, and 2.14%±1.60%, respectively. The inter-operative variation for endocardium, mid-wall and epicardial layers was 4.53%±1.64%, 4.93%±1.72%, and 4.79%±1.63%, respectively. The reason for the variation is due to the differences in segmentation results of endocardium and epicardium.
Discussion
3D twist computation has the potential to overcome the out-of-plane error and plane selection difficulties, as well as producing more reliable LV twist indices. The value of twist is not the same in epicardium, midwall and endocardium.
Cardiac twist
LV twisting value gradually increases in the aging process. This finding is in accordance with previous tagged MRI experiments, as well as 2D speckle tracking studies published in independent studies (19-21). The peak basal and apical twist, computed by 2D STE, is not the same in the literature which is confusing to the readers. Takeuchi et al. (20) reported a twist value in the range of 6-7 degrees, lower than the LV peak twist reported in our study (10-19 degrees). However, Lee et al. (21) and Sun et al. (15) reported peak twist values in the range of 20 degrees, closer to the studies in this paper. Tagged MRI experiments have resulted in twist rates in the range of 16-20 (closer to the studies performed in this article) (20,21). The myocardial fibrosis and molecular changes of the heart can be responsible for the age related twist changes (22).
Correlation of 0.31 for age and twist is meaningful but weak. We hypothesize that the reason for the weak correlation is the large variation in the aging process among the subjects. Interestingly, Sun et al. (15) achieved a correlation ratio of 0.33, which is close to our results. In our previous study in 3D echocardiography images (17), we achieved a correlation ratio of (r=0.3074); which is very close to the correlation ratio measured in this study (0.31407). The twist values for 3D echocardiography images are not exactly similar to the twist values for 3D tagged MRI images. A comparison of the computed twist values for tagged MRI in this article and echocardiography twist values in (17) shows a correlation ratio of r=0.94.
We hypothesize that the sources of the discrepancy between different articles might be sensitivity of 2D STE to out-of-plane error and plane selection differences. Advances in the field of imaging system, using different softwares for analysis, and different age groups of patients can be other reasons.
Limitations of the study
Tag lines fade over time and are not as sharp in end diastole and lead to less accurate motion vectors. Exclusion of the obese subjects and poor quality of some of the tagged MR images can be considered another limitation of this study. Additionally, it is not possible to segment the subendocardium and subepicardium in tagged MR images based on real fiber directions. The resolution of the tagged MR images is not the same in the x, y and z directions and the discrepancy in the resolution in different directions can lead to error. Imaging artifacts can also decrease the accuracy of twist analysis. Finally, tagged MR acquisition necessitates breath holding/gating and EKG gating and, therefore, heart rate and cardiac variability can cause error (23).
Conclusions
Three-dimensional motion detection in tagged MR images is a feasible method for twist rate measurements. However, external factors such as age can change the displacement values; aging increases the global systolic LV twist. This may be the result of sub-endocardial fibrosis and malfunction caused by the aging process. LV apex rotates with respect to the LV base during systole. As seen from the LV apex, systolic apical rotation is counterclockwise and basal rotation is clockwise, causing torsion in the long axis dimension. This is the first study to compute 3D LV twist for different cardiac layers in a large group of subjects using tagged MR data.
Acknowledgements
Disclosure: Authors do not have any financial interest or collaboration with companies.
References
- 1.Hansen DE, Daughters GT, 2nd, Alderman EL, et al. Effect of volume loading, pressure loading, and inotropic stimulation on left ventricular torsion in humans. Circulation 1991;83:1315-26 [DOI] [PubMed] [Google Scholar]
- 2.Moon MR, Ingels NB, Jr, Daughters GT, 2nd, et al. Alterations in left ventricular twist mechanics with inotropic stimulation and volume loading in human subjects. Circulation 1994;89:142-50 [DOI] [PubMed] [Google Scholar]
- 3.Buchalter MB, Rademakers FE, Weiss JL, et al. Rotational deformation of the canine left ventricle measured by magnetic resonance tagging: effects of catecholamines, ischaemia, and pacing. Cardiovasc Res 1994;28:629-35 [DOI] [PubMed] [Google Scholar]
- 4.Young AA, Cowan BR. Evaluation of left ventricular torsion by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2012;14:49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dong SJ, Hees PS, Siu CO, et al. MRI assessment of LV relaxation by untwisting rate: a new isovolumic phase measure of tau. Am J Physiol Heart Circ Physiol 2001;281:H2002-9 [DOI] [PubMed] [Google Scholar]
- 6.Amundsen BH, Helle-Valle T, Edvardsen T, et al. Noninvasive myocardial strain measurement by speckle tracking echocardiography: validation against sonomicrometry and tagged magnetic resonance imaging. J Am Coll Cardiol 2006;47:789-93 [DOI] [PubMed] [Google Scholar]
- 7.Notomi Y, Lysyansky P, Setser RM, et al. Measurement of ventricular torsion by two-dimensional ultrasound speckle tracking imaging. J Am Coll Cardiol 2005;45:2034-41 [DOI] [PubMed] [Google Scholar]
- 8.Grabskaya E, Spira C, Hoffmann R, et al. Myocardial rotation but not circumferential strain is transducer angle dependent: a speckle tracking echocardiography study. Echocardiography 2010;27:809-14 [DOI] [PubMed] [Google Scholar]
- 9.Sengupta PP, Tajik AJ, Chandrasekaran K, et al. Twist mechanics of the left ventricle: principles and application. JACC Cardiovasc Imaging 2008;1:366-76 [DOI] [PubMed] [Google Scholar]
- 10.Tavakoli V, Sahba N, Ahmadian A, et al. Adaptive multi-resolution myocardial motion analysis of b-mode echocardiography images using combined local/global optical flow. IEEE proceeding on Bioinformatics and Biomedical Engineering (iCBBE), 2008:2033-6. [Google Scholar]
- 11.Tavakoli V, Nambakhsh MS, Sahba N, et al. A new variational technique for combining affine registration and optical flow in echocardiography images. 30th Annual IEEE Engineering in Medicine and Biology conference (EMBS) 2008:205-08. [DOI] [PubMed] [Google Scholar]
- 12.Tavakoli V, Sahba N.Assessment of age-related changes in left ventricular twist by 3-dimensional speckle-tracking echocardiography. J Ultrasound Med 2013;32:1435-41 [DOI] [PubMed] [Google Scholar]
- 13.Tavakoli V, Amini AA. A Survey of Shaped-Based Registration and Segmentation Techniques for Cardiac Images. Comput Vis Image Underst 2013;117:966-89 [Google Scholar]
- 14.Pan L, Prince JL, Lima JA, et al. Fast tracking of cardiac motion using 3D-HARP. IEEE Trans Biomed Eng 2005;52:1425-35 [DOI] [PubMed] [Google Scholar]
- 15.Sun JP, Lam YY, Wu CQ, et al. Effect of age and gender on left ventricular rotation and twist in a large group of normal adults - A multicenter study. Int J Cardiol 2013;167:2215-21 [DOI] [PubMed] [Google Scholar]
- 16.Zhang Y, Zhou QC, Pu DR, et al. Differences in left ventricular twist related to age: speckle tracking echocardiographic data for healthy volunteers from neonate to age 70 years. Echocardiography 2010;27:1205-10 [DOI] [PubMed] [Google Scholar]
- 17.Tavakoli V, Sahba N.Assessment of age-related changes in left ventricular twist by 3-dimensional speckle-tracking echocardiography. J Ultrasound Med 2013;32:1435-41 [DOI] [PubMed] [Google Scholar]
- 18.Mor-Avi V, Lang RM, Badano LP, et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. Eur J Echocardiogr 2011;12:167-205 [DOI] [PubMed] [Google Scholar]
- 19.Tavakoli V, Sahba N.Cardiac motion and strain detection using 4D CT images: comparison with tagged MRI, and echocardiography. Int J Cardiovasc Imaging 2014;30:175-84 [DOI] [PubMed] [Google Scholar]
- 20.Takeuchi M, Nakai H, Kokumai M, et al. Age-related changes in left ventricular twist assessed by two-dimensional speckle-tracking imaging. J Am Soc Echocardiogr 2006;19:1077-84 [DOI] [PubMed] [Google Scholar]
- 21.Lee HJ, Kim BS, Kim JH, et al. Age-related changes in left ventricular torsion as assessed by 2-dimensional ultrasound speckle tracking imaging. Korean Circ J 2008;38:529-35 [Google Scholar]
- 22.Goffinet C, Chenot F, Robert A, et al. Assessment of subendocardial vs. subepicardial left ventricular rotation and twist using two-dimensional speckle tracking echocardiography: comparison with tagged cardiac magnetic resonance. Eur Heart J 2009;30:608-17 [DOI] [PubMed] [Google Scholar]
- 23.Olivetti G, Giordano G, Corradi D, et al. Gender differences and aging: effects on the human heart. J Am Coll Cardiol 1995;26:1068-79 [DOI] [PubMed] [Google Scholar]