

Abstract
Contrast-induced nephrotoxicity (CIN) is a form of acute kidney injury that follows intravascular contrast media exposure. CIN may be preventable because its risk factors are well established and the timing of renal insult is commonly known in advance. However, contrast-induced nephrotoxicity is still the third leading cause of iatrogenic renal failure. This important complication accounts up to 10% of acute renal failure cases in hospitalized patients and it is associated with increased short- and long-term morbidity and mortality. Prolonged hospitalization follows and overall increases healthcare resource utilization. This paper will discuss the various prophylactic procedures tested in clinical trials.
1. Introduction
The general indication for the use of radiographic contrast agents is to enhance images in diagnostic and therapeutic interventions. Increasing use of contrast media (CM) during radiological procedures has resulted in an increasing incidence of contrast-induced nephrotoxicity (CIN). In the year 2003, about 8 million liters of contrast media was used in 80 million contrast media examinations [1]. This makes it one of the highest volumes of medical drugs used. Development of contrast-induced nephrotoxicity (CIN) is a common complication of radiocontrast media exposure in patients who possess underlying risk factors.
2. Definition of CIN
The definition of CIN varies widely and refers to the development of acute renal impairment following the intravascular administration of radiocontrast dye in the absence of other identifiable causes of renal failure. Typically it occurs within 24–48 hours after administration of contrast media and peaks by day 5 after exposure [1, 2]. The most commonly used definition is an increase of more than ≥25% in serum creatinine level (SCr) or an absolute increase of 0.5 mg/dL (44.2 μmol/L) from baseline value [1–5]. CIN corresponds to one stage increase in the 3 stages according to the KDIGO acute kidney injury network criteria [6].
3. Risk Factors for Contrast-Induced Nephrotoxicity
Risk factors for the development of CIN have been examined in several studies and can be divided into patient-related and non-patient-related factors. The patient-related risk factors include preexisting renal dysfunction, diabetes mellitus, multiple myeloma, advanced age, congestive heart failure, hemodynamic instability, hypertension, hypotension, emergency procedure, anaemia, left ventricular ejection fraction <40%, nephrotic syndrome, and myocardial infarction [3, 7]. The non-patient-related risk factors are volume, osmolality, ionicity and viscosity of the contrast media, intra-arterial versus intravenous injection, concomitant use of nephrotoxic drugs, and volume depletion [7, 8]. The most important risk factor for CIN is chronic kidney disease (CKD). Generally, the estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 is considered a cut-off value for increased risk for CIN (2%) [8]. The lower the eGFR value is, the greater the risk of CIN is. It is fivefold higher (10.2%), if serum creatinine is in the range 1.4–1.9 mg/dL [3]. The majority of the studies on CIN were performed on patients undergoing cardiac procedure following intra-arterial CM administration. Thus, one conclusion was therefore that intra-arterial CM administration leads to a higher risk of CIN as compared to an intravenous study population [9, 10]. The only one head-to-head study available to date comparing intravenous route with intra-arterial route found is the study of Karlsberg et al. This study showed that intravenous route might be as nephrotoxic as intra-arterial route; even the dose of applied CM was higher. So most of the intra-arterial injections are mainly intravenous for the kidney [11]. Volume of contrast media seems to be a major procedure-related risk factor of CIN. Therefore, the use of volume-to-creatinine clearance ratio (v/CrCl) can be used as an index for prediction of an abnormal increase in postinterventional creatinine. A ratio of the CM volume to the creatinine clearance below 2.62 has been suggested as a safe limit [12, 13]. But a “safe” dose does not exist and even very limited doses of CM may cause CIN in high-risk patients. The likelihood of CIN rises sharply as the number of risk factors increases. Cystatin C appears to be a good biomarker in the prediction of acute kidney injury, but so far it is almost not used to detect CIN [14]. Other new biomarkers such as neutrophil gelatinase-associated lipocalin (NGAL) are not helpful to better diagnose CIN [15]. Studies testing KIM-1 are inconsistent because of the small number of studies and heterogeneity between them [16].
4. Prevention for CIN
4.1. Hydration
Hydration only is the intervention best supported by evidence with a preventive effect on CIN, though no randomized controlled trials directly compared hydration versus no hydration. Intravenous hydration seems to be more effective than unrestricted oral hydration [17]. Standardized prospective studies to determine the optimal hydration strategy are needed. Several potential mechanisms can contribute to the beneficial effect of volume expansion, including dilution of contrast media within the tubule lumen, increased diuresis, reduced activation of renin-angiotensin system due to increased delivery of sodium to the distal nephron, and minimizing of the renal production of nitric oxide [18]. Solomon et al. were the first who showed the positive effect of adequate hydration [19]. Contrasting the Solomon study, others and we found that furosemide was beneficial. Furosemide was given after CM and not before it in our study; in the other studies the urine output rate should be >300 mL/h [20, 21]. The high urine output and positive fluid balance in combination with furosemide to keep the high-risk patients euvolemic is controlled by the RenalGuard system. These studies are promising but investigator driven [23, 24]. In addition to timing and route of hydration, other factors, such as fluid composition, may also play a role. In a randomized trial that included 1620 patients, Mueller et al. showed that intravenously administered 0.9% saline solution was superior to 0.45% saline solution [22]. Furthermore, two small studies suggest that sustained fluid administration intravenously within 12 h before and 12 h after administration of contrast media is superior to bolus administration at the time of contrast administration [25, 26]. CIN Consensus Working Panel recommendations published in 2006 suggested adequate intravenous volume expansion with isotonic crystalloid (1.0–1.5 mL/kg/hr) for 3 to 12 hr before the procedure and continued for 6 to 24 hr to prevent CIN in patients at risk [27].
4.2. Vasodilators
Renal vasodilatators, including calcium-channel antagonists, are promising agents in the prevention of CIN. So far their administration has failed to show conclusive evidence of a beneficial effect [28, 29]. Given its dilatory effect on the renal vasculature and the ability to increase renal blood flow and GFR, dopamine was supposed to be useful in the prevention of CIN. This hypothesis was evaluated in several studies and none showed a benefit in terms of dopamine administration [30–32]. Fenoldopam, a selective dopamine-1 receptor agonist with vasodilatory properties, was unable to lower the risk of CIN in a small population [33–35]. Critical experts argue that the doses of dopamine and fenoldopam used in these trials may have been insufficient to produce renal vasodilatation [36]. The adverse effects of these drugs were arrhythmia with dopamine and hypotension associated with intravenous fenoldopam administration. Small underpowered trials using vasodilating agents such as natriuretic peptide [37], an endothelin antagonist [38], prostaglandin E1 [39], angiotensin converting enzyme inhibitors [40], and L-arginine [41] have shown no benefit and in some cases even a potential harm [41].
4.3. Sodium Bicarbonate
Sodium bicarbonate may be an effective therapy for the prevention of contrast-induced nephrotoxicity [42]. The proposed mechanisms are that alkalinizing the tubular urine with sodium bicarbonate infusion may attenuate free radical formation and oxidant injury. Merten et al. presented the first study to prevent CIN by the administration of bicarbonate solution in a concentration of 154 mMol/L. In this study, the administration of bicarbonate was associated with a decreased incidence of CIN [43]. Subsequent studies have failed to show any additional benefit of the intravenous administration of sodium bicarbonate over isotonic sodium chloride alone in CIN prevention; also these studies had a dose reduction of NaHCO3 [44, 45]. In a systematic overview of 14 randomized trials, 2290 patients were included comparing sodium bicarbonate with sodium chloride for the prevention of CIN. Of those trials three were categorized as large (n = 1145) and 12 as small (n = 1145). Among the large trials, the CIN incidence for sodium bicarbonate and sodium chloride was 10.7 and 12.5%, respectively; the relative risk (RR) with 95% confidence interval (CI) was 0.85 (0.63 to 1.16) without evidence of heterogeneity (P = 0.09, I(2) = 0%). The pooled RR (95% CI) among the 12 small trials was 0.50 (0.27 to 0.93) with significant between-trial heterogeneity (P = 0.01; I(2) = 56%). The small trials were more likely to show a benefit for hydration with sodium bicarbonate, but these studies were generally of lower methodological quality. Among the larger, randomized trials, there was no statistically significant difference between hydration with sodium bicarbonate and sodium chloride. These data suggest that the true clinical benefit of hydration with sodium bicarbonate, if any, is likely to be small for the average patient [46–50].
4.4. Antioxidant: N-Acetylcysteine
The use of N-acetylcysteine, an agent with antioxidant properties, in the prevention of CIN is based on the assumption that CIN is caused by reactive oxygen species (ROS). ROS presumably are formed as a result of direct toxic effect of contrast media on tubular epithelial cells. Tepel et al. conducted the first study [51], showing that serum creatinine levels rose by more than 0.5 mg/dL in only 2% of patients who received N-acetylcysteine (600 mg bid orally) as compared to 21% of patients in the control group (P < 0.001). In the control group, 9 patients needed dialysis but only 1 in the N-acetylcysteine group. Many other studies on N-acetylcysteine followed; one of the latest is the large study of Berwanger and the ACT Investigators published in 2011. This study showed no benefit using N-acetycysteine p.o. in the incidence of CIN reduction as well as other clinically relevant outcomes [52]. Several meta-analyses showed no significant benefits of N-acetylcysteine (600 mg bid orally) compared to controls [53, 54]. Thus, the meta-analyses of N-acetylcysteine trials have led to disparate conclusions. The latest report included 22 trials with 2746 patients. There was a significant heterogeneity among those trials (I (2) = 37%; P = 0.04), but meta-regression analysis failed to identify significant sources of heterogeneity. Two clusters were studied: cluster 1 (n = 18; 2445 patients) showed no benefit where the relative risk (RR) was 0.87 and the 95% confidence interval (CI) 0.68–1.12 (P = 0.28). The studies in cluster 2 (n = 4; 301 patients) indicated that N-acetylcysteine was highly beneficial (RR = 0.15; 95% CI 0.07–0.33, P < 0.0001). However, cluster 2 studies were relatively early, small, and of lower quality compared with cluster 1 studies (P = 0.01 for the three factors combined). Need for dialysis across all studies (5 in control group and 8 in the treatment group, P = 0.42) did not suggest that N-acetylcysteine is beneficial [55, 56]. The dose of N-acetylcysteine that has been investigated might be too low to achieve meaningful ROS reduction. Briguori et al. compared therefore standard dose (600 mg bid orally) versus high doses (1200 mg bid orally) on the day of procedure [57]; the rate of CIN was lower in patients receiving high-dose N-acetylcysteine (4% versus 11%; P = 0.03). The benefit of high-dose N-acetylcysteine versus intravenous hydration was even more pronounced in the study by Baker et al., where N-acetylcysteine was given intravenously immediately before contrast agent [58]. CIN occurred in 2 patients in the N-acetylcysteine group (5%) and in 8 patients in the hydration group (21%, P = 0.045). Therefore, this high intravenous dose protocol can be used for all emergency patients or outpatients at the same day. Further investigations for such protocols are needed (Table 1).
Table 1.
Agents and measures proposed for prevention of contrast-agent-induced nephrotoxicity.
| Drug | Trial | Patients | Prophylactic benefit | Reference |
|---|---|---|---|---|
| Mesna | RCT | N = 100 | Yes | [59] |
|
| ||||
| NAC | RCT Meta-analysis |
N = 83 N = 2746 |
Yes Equivocal |
[51] [55, 56] |
|
| ||||
| Hydration | RCT RCT |
N = 78 N = 1620 N = 53 |
Yes Yes Yes |
[19] [22] [17] |
|
| ||||
| Sodium bicarbonate |
RCT RCT Meta-analysis |
N = 119 N = 353 N = 2290 |
Yes No Equivocal |
[43] [44] [46] |
|
| ||||
| Theophyllin | Meta-analysis | N = 585 | No | [60] |
4.5. Antioxidant: Mesna
Mesna (mercaptoethane-sulfonate Na), an agent with antioxidant properties, can reduce free radicals and restore reduced glutathione (GSH) levels after ischemic renal failure [61]. An advantage of Mesna is its 60% elimination by glomerular filtration (Figure 1), whereas N-acetylcysteine is less than 10% excreted in the urine [59]. There is so far only one single randomized controlled trial by our group, which investigated the use of Mesna in prevention of contrast-induced nephrotoxicity. In our study we compared the efficacy of intravenous administration of 1600 mg Mesna versus placebo in addition to intravenous hydration with 0.9% saline. The results were a CIN in 7 patients in the placebo group and none in the Mesna group. The immediate preinvestigational infusion makes Mesna easy to use in outpatients as well as for emergency procedures. Clearly, the investigation by a multicenter trial is needed to confirm the benefit of Mesna.
Figure 1.
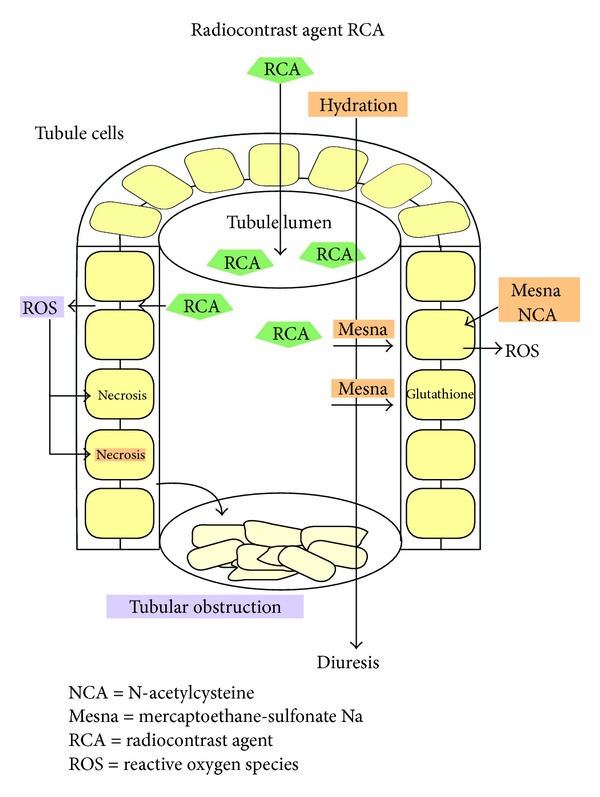
Presumed renoprotective effects of Mesna in tubule lumen. Radiocontrast agents (RCA) are filtered into the primary urine. In the tubule lumen, RCAs are concentrated 100-fold by water reabsorption. High RCA concentration stimulates the production of reactive oxygen (ROS) in the tubule cells leading to epithelial cell necrosis and tubule obstruction. By hydration, RCAs are less concentrated and tubule obstruction can be washed out. While N-acetylcysteine acts mainly from the basal side, Mesna can prevent ROS production in the tubule cells from both apical and basal sides. Finally Mesna may prevent contrast-agent-induced nephrotoxicity by glutathione regeneration. Graphic: G.Hintze.
4.6. Antioxidant: Ascorbic Acid
Ascorbic acid can reduce free radical production. Oral ascorbic acid (3 g before and 2 g twice after the procedure) was evaluated in a randomized controlled trial that included 231 patients [62]. The incidence in contrast-induced nephrotoxicity was 9% in the ascorbic acid group and 20% in the placebo group (P = 0.02). In a recently published meta-analysis Sadat et al. showed that in 1536 patients, who completed the trial, ascorbic acid produced a 33% lower risk of developing a CIN [63]. So ascorbic acid might be a form of prophylactic regime in contrast media induced renal failure; nevertheless it has not been recommended by the CM safety committee.
4.7. Theophylline
There are only small studies of theophylline as a potential prophylactic agent for CIN with conflicting results. Nine trials (n = 585 patients) compared theophylline with no active treatment. Meta-analysis identified considerable heterogeneity among these studies [60]. There was variability in the inclusion criteria, the method, and schedule of theophylline administration and hydration protocols as well as in the type of contrast media. Only few trials compared the incidence of adverse events. To date there is no supporting evidence for the use of theophylline for the prevention of CIN.
4.8. Atrial Natriuretic Peptide
Atrial natriuretic peptide failed to prevent CIN in a randomized, placebo-controlled study of Kurnik et al. [37].
4.9. Statins
Statins have been shown to have pleiotropic, antioxidant, and anti-inflammatory effects. In a retrospective register study of 29409 patients who underwent percutaneous coronary angiography, statin therapy before the procedure was linked with a lower incidence of CIN compared to patients not taking a statin at that time [64]. These results are in line with a prospective, observational study that included 434 participants. Patients who were taking statins before undergoing coronary angiography had a lower rate of CIN [65]. However, later ongoing trials with simvastatin in the PROMISS study [66] and in the diabetes subgroup failed to demonstrate benefits of treatment as well as with atorvastatin [67]. Another trial has been started with high-loading dose of atorvastatin (80 mg); in this small study the results show a benefit for patients receiving the high-loading dose compared to placebo (CIN: 5% versus 13.2%, P = 0.046) [68]. In the multivariable analysis, atorvastatin pretreatment was independently associated with a decreased risk of CIN (odds ratios 0.34, 95% confidence interval 0.12 to 0.97, P = 0.043) and shortening of hospital days [68]. Quintavalle et al. demonstrated in a single centre prospective study with 410 patients that a single high-loading dose of atorvastatin (80 mg within 24 hours before contrast media exposure) significantly reduced the risk of contrast-induced nephropathy (4.5% versus 17.8%). This effect was only obvious in patients with moderate risk and a glomerular filtration rate between 31 and 60 mL/min. The definition of contrast-induced renal failure is new, since cystatin C as marker was used [69]. The study was not powered to detect an effect according to the more traditional and less sensitive definition of contrast-induced acute kidney injury [70]. Another interesting approach was made with the substance rosuvastatin. Leoncini et al. could demonstrate that a high-dose rosuvastatin (40 mg given on admission to statin-naïve patients with ACS, followed by 20 mg/day) compared to no statin treatment reduced the risk of CIN significantly (6.7% versus 15.1%; adjusted odds ratio: 0.38; 95% confidence interval (CI): 0.20 to 0.71; P = 0.003). In this interesting study the benefit of rosuvastatin was consistent, even applying different definitions of contrast-induced nephropathy. It showed even after 6-month follow-up further benefit with lower rate of death or nonfatal myocardial infarction [71].So since the substances are heterogeneous as well as the dose, further investigations are needed.
4.10. Hemodialysis and Hemofiltration
Several studies examined the effect of hemodialysis, immediately after exposure to contrast media to prevent the further deterioration of renal function in patients with preexisting advanced renal disease. Theoretically, hemodialysis is an effective method in removing contrast media from the patient's body. One study of removing contrast media via hemodialysis was even performed during coronary intervention in patients with advanced renal insufficiency, but no significant effect on renal function was observed compared with patients who did not undergo hemodialysis [72]. Paradoxically, in a study reported by Vogt et al. hemodialysis performed after CM administration was associated with a significantly greater mean peak in serum creatinine (P < 0.05) compared with patients who did not undergo hemodialysis [73, 74]. Finally, patients with end-stage renal failure who underwent a 6-hour hemodialysis postprocedure were without a benefit [75]. On the basis of these data, hemodialysis cannot be recommended.
Two studies [76, 77] investigated the effect of continuous venovenous hemofiltration for prevention of CIN in patients with chronic renal insufficiency as compared with intravenous hydration. A >25% increase of creatinine and the in-hospital mortality were significantly lower in the hemofiltration group. However, since creatinine level is naturally influenced by hemofiltration, assessment of benefit in prevention on CIN based on this endpoint is certainly debatable. The benefits of hemofiltration observed in this study have been suggested to be due to the concomitant administration of heparin, which has anti-inflammatory effects and might reduce ROS generation. A different mechanism that might play a role was high-volume controlled hydration before contrast media exposure [77]. This method deserves further investigations; nevertheless, it is expensive and invasive.
5. Contrast Media Use
Contrast media are classified according to osmolality, which reflects the total particle concentration of the solution. High-osmolar contrast media (HOCM) have about 1500 to 1800 mOsmol/kg osmolality. Low-osmolar contrast media (LOCM) have 600 to 800 mOsm/kg and isoosmolar contrast media (IOCM) 290 mOsm/kg. In a meta-analysis of comparative trials [78], an increase in serum creatinine of more than 0.5 mg/dL after administration of contrast media was less frequent with low-osmolar than with high-osmolar contrast media (odds ratio, 0.5; 95% confidence interval, 0.36 to 0.68). Thus in western countries HOCM have been completely replaced by LOCM due to the lower incidence of side effects from LOCM with no difference in image quality. In a recently published systematic overview of 36 randomized, controlled trials (n = 7166 patients) nephrotoxicity of isoosmolar contrast media iodixanol (n = 3672) was compared to diverse low-osmolar contrast media (n = 3494). In this analysis [79], iodixanol showed no statistically significant reduction in the incidence of contrast-induced nephrotoxicity below that observed with heterogeneous comparator agents. Since molecular weight of isoosmolar agents is higher (1550 daltons versus 750–850 daltons in low-osmolar agents), they have a higher viscosity and likely therefore no significant benefit could be shown in any high-risk subgroups; there was only a significant benefit of iodixanol when compared with iohexol [79]. So the CM safety committee (GMSC) guidelines recommend the use of LOCM and IOCM in patients with risk factors for CIN [80].
6. Summary and Recommendations
Contrast-induced nephrotoxicity is a serious adverse event for which preventive care is needed since treatment options are of limited value. Physicians using contrast media should incorporate preventive strategies into their clinical practices. The consulting nephrologists can provide guidance to radiologists and cardiologists regarding the identification of patients at risk and suggest the best practical strategy to reduce the incidence of CIN.
These practical measures include the assessment of patients at risk. Patients with normal kidney function and without risk factor for contrast-induced nephrotoxicity do not require prophylactic intervention before contrast media use. Patients with underlying renal dysfunction and an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 have to be identified particularly in combination with other risks which have to be identified. Potentially nephrotoxic drugs (NSAIDs) as well as metformin should be withdrawn before contrast administration. The use of the lowest contrast volume as possible is recommended and high-osmolar contrast media should be avoided. The best way to prevent CIN is to provide adequate periprocedural hydration. The role of various drugs in prevention of CIN (such as Mesna) is still controversial and warrants future studies.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
References
- 1.Katzberg RW, Haller C. Contrast-induced nephrotoxicity: clinical landscape. Kidney International. 2006;69:S3–S7. doi: 10.1038/sj.ki.5000366. [DOI] [PubMed] [Google Scholar]
- 2.Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. The American Journal of Kidney Diseases. 2002;39(5):930–936. doi: 10.1053/ajkd.2002.32766. [DOI] [PubMed] [Google Scholar]
- 3.Mehran R, Nikolsky E. Contrast-induced nephropathy: definition, epidemiology, and patients at risk. Kidney International. 2006;69:S11–S15. doi: 10.1038/sj.ki.5000368. [DOI] [PubMed] [Google Scholar]
- 4.Lasser EC, Lyon SG, Berry CC. Reports on contrast media reactions: analysis of data from reports to the U.S. Food and Drug Administration. Radiology. 1997;203(3):605–610. doi: 10.1148/radiology.203.3.9169676. [DOI] [PubMed] [Google Scholar]
- 5.Berg KJ. Nephrotoxicity related to contrast media. Scandinavian Journal of Urology and Nephrology. 2000;34(5):317–322. doi: 10.1080/003655900750048341. [DOI] [PubMed] [Google Scholar]
- 6.Lameire N, Kellum JA, KDIGO AKI Guideline Work Group Contrast-induced acute kidney injury and renal support for acute kidney injury: a KDIGO summary (Part 2) Critical Care. 2013;17, article 205 doi: 10.1186/cc11455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pucelikova T, Dangas G, Mehran R. Contrast-induced nephropathy. Catheterization and Cardiovascular Interventions. 2008;71(1):62–72. doi: 10.1002/ccd.21207. [DOI] [PubMed] [Google Scholar]
- 8.Pannu N, Wiebe N, Tonelli M. Prophylaxis strategies for contrast-induced nephropathy. Journal of the American Medical Association. 2006;295(23):2765–2779. doi: 10.1001/jama.295.23.2765. [DOI] [PubMed] [Google Scholar]
- 9.Katzberg RW, Lamba R. Contrast-induced nephropathy after intravenous administration: fact or fiction? Radiologic Clinics of North America. 2009;47(5):789–800. doi: 10.1016/j.rcl.2009.06.002. [DOI] [PubMed] [Google Scholar]
- 10.Kim SM, Cha RH, Lee JP, et al. Incidence and outcomes of contrast-induced nephropathy after computed tomography in patients with CKD: a quality improvement report. The American Journal of Kidney Diseases. 2010;55(6):1018–1025. doi: 10.1053/j.ajkd.2009.10.057. [DOI] [PubMed] [Google Scholar]
- 11.Karlsberg RP, Dohad SY, Sheng R. Contrast mediuminduced acute kidney injury: comparison of intravenous and intraarterial administration of iodinated contrast medium. Journal of Vascular and Interventional Radiology. 2011;22(8):1159–1165. doi: 10.1016/j.jvir.2011.03.020. [DOI] [PubMed] [Google Scholar]
- 12.Laskey WK, Jenkins C, Selzer F, et al. Volume-to-creatinine clearance ratio: a pharmacokinetically based risk factor for prediction of early creatinine increase after percutaneous coronary intervention. Journal of the American College of Cardiology. 2007;50(7):584–590. doi: 10.1016/j.jacc.2007.03.058. [DOI] [PubMed] [Google Scholar]
- 13.Tan N, Liu Y, Zhou YL, et al. Contrast medium volume to creatinine clearance ratio: a predictor of contrast-induced nephropathy in the first 72 hours following percutaneous coronary intervention. Catheterization and Cardiovascular Interventions. 2011;79(1):70–75. doi: 10.1002/ccd.23048. [DOI] [PubMed] [Google Scholar]
- 14.Zhang Z, Lu B, Sheng X, Jin N. Cystatin C in prediction of acute kidney injury: a systemic review and meta-analysis. The American Journal of Kidney Diseases. 2011;58(3):356–365. doi: 10.1053/j.ajkd.2011.02.389. [DOI] [PubMed] [Google Scholar]
- 15.Valette X, Sarary B, Nowoczyn M, et al. Accuracy of plasma neutrophil gelatinase-associated lipocalin in the early diagnosis of contrast-induced acute kidney injury in critical illness. Intensive Care Medicine. 2013;39:857–865. doi: 10.1007/s00134-013-2826-y. [DOI] [PubMed] [Google Scholar]
- 16.Shao X, Tian L, Xu W, et al. Diagnostic value or urinary kidney injury molecule 1 for acute kidney injury: a meta-analysis. PLoS ONE. 2014;9 doi: 10.1371/journal.pone.0084131.e84131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Trivedi HS, Moore H, Nasr S, et al. A randomized prospective trial to assess the role of saline hydration on the development of contrast nephrotoxicity. Nephron. Clinical practice. 2003;93(1):C29–C34. doi: 10.1159/000066641. [DOI] [PubMed] [Google Scholar]
- 18.McCullough PA, Adam A, Becker CR, et al. Risk prediction of contrast-induced nephropathy. The American Journal of Cardiology. 2006;98(6):27–36. doi: 10.1016/j.amjcard.2006.01.022. [DOI] [PubMed] [Google Scholar]
- 19.Solomon R, Werner C, Mann D, D’Elia J, Silva P. Effects of saline, mannitol, and furosemide on acute decreases in renal function induced by radiocontrast agents. The New England Journal of Medicine. 1994;331(21):1416–1420. doi: 10.1056/NEJM199411243312104. [DOI] [PubMed] [Google Scholar]
- 20.Lukas R, Eren A, Zellner D, et al. Furosemide after contrast media does no harm to the kidneys and allows for preventive hydration. Perfusion. 2003;16:326–333. [Google Scholar]
- 21.Marenzi G, Ferrari C, Marana I, et al. Prevention of contrast nephropathy by furosemide with matched hydration: the MYTHOS (induced diuresis with matched hydration compared to standard hydration for contrast induced nephropathy prevention) trial. JACC: Cardiovascular Interventions. 2012;5(1):90–97. doi: 10.1016/j.jcin.2011.08.017. [DOI] [PubMed] [Google Scholar]
- 22.Solomon R. Forced diuresis with the RenalGuard system: impact on contrast induced acute kidney injury. Journal of Cardiology. 2014;63:9–13. doi: 10.1016/j.jjcc.2013.10.001. [DOI] [PubMed] [Google Scholar]
- 23.Briguori C. Renalguard system: a dedicated device to prevent contrast-induced acute kidney injury. International Journal of Cardiology. 2012;6:291–297. doi: 10.1016/j.ijcard.2011.12.069. [DOI] [PubMed] [Google Scholar]
- 24.Mueller C, Buerkle G, Buettner HJ, et al. Prevention of contrast media-associated nephropathy: randomized comparison of 2 hydration regimens in 1620 patients undergoing coronary angioplasty. Archives of Internal Medicine. 2002;162(3):329–336. doi: 10.1001/archinte.162.3.329. [DOI] [PubMed] [Google Scholar]
- 25.Bader BD, Berger ED, Heede MB, et al. What is the best hydration regimen to prevent contrast media-induced nephrotoxicity? Clinical Nephrology. 2004;62(1):1–7. doi: 10.5414/cnp62001. [DOI] [PubMed] [Google Scholar]
- 26.Krasuski RA, Beard BM, Geoghagan JD, Thompson CM, Guidera SA. Optimal timing of hydration to erase contrast-associated nephropathy: the OTHER CAN study. Journal of Invasive Cardiology. 2003;15(12):699–702. [PubMed] [Google Scholar]
- 27.Stacul F, Adam A, Becker CR, et al. Strategies to Reduce the Risk of Contrast-Induced Nephropathy. The American Journal of Cardiology. 2006;98(6):59–77. doi: 10.1016/j.amjcard.2006.01.024. [DOI] [PubMed] [Google Scholar]
- 28.Khoury Z, Schlicht JR, Como J, et al. The effect of prophylactic nifedipine on renal function in patients administered contrast media. Pharmacotherapy. 1995;15(1):59–65. [PubMed] [Google Scholar]
- 29.Madsen JK, Jensen LW, Sandermann J, et al. Effect of nitrendipine on renal function and on hormonal parameters after intravascular iopromide. Acta Radiologica. 1998;39(4):375–380. doi: 10.1080/02841859809172448. [DOI] [PubMed] [Google Scholar]
- 30.Gare M, Haviv YS, Ben-Yehuda A, et al. The renal effect of low-dose dopamine in high-risk patients undergoing coronary angiography. Journal of the American College of Cardiology. 1999;34(6):1682–1688. doi: 10.1016/s0735-1097(99)00422-2. [DOI] [PubMed] [Google Scholar]
- 31.Hans SS, Hans BA, Dhillon R, Dmuchowski C, Glover J. Effect of dopamine on renal function after arteriography in patients with pre-existing renal insufficiency. The American Surgeon. 1998;64(5):432–436. [PubMed] [Google Scholar]
- 32.Weisberg LS, Kurnik PB, Kurnik BRC. Risk of radiocontrast nephropathy in patients with and without diabetes mellitus. Kidney International. 1994;45(1):259–265. doi: 10.1038/ki.1994.32. [DOI] [PubMed] [Google Scholar]
- 33.Allaqaband S, Tumuluri R, Malik AM, et al. Prospective randomized study of N-acetylcysteine, fenoldopam, and saline for prevention of radiocontrast-induced nephropathy. Catheterization and Cardiovascular Interventions. 2002;57(3):279–283. doi: 10.1002/ccd.10323. [DOI] [PubMed] [Google Scholar]
- 34.Stone GW, McCullough PA, Tumlin JA, et al. Fenoldopam mesylate for the prevention of contrast-induced nephropathy: a randomized controlled trial. Journal of the American Medical Association. 2003;290(17):2284–2291. doi: 10.1001/jama.290.17.2284. [DOI] [PubMed] [Google Scholar]
- 35.Tumlin JA, Wang A, Murray PT, Mathur VS. Fenoldopam mesylate blocks reductions in renal plasma flow after radiocontrast dye infusion: a pilot trial in the prevention of contrast nephropathy. The American Heart Journal. 2002;143(5):894–903. doi: 10.1067/mhj.2002.122118. [DOI] [PubMed] [Google Scholar]
- 36.Teirstein PS, Price MJ, Mathur VS, Madyoon H, Sawhney N, Baim DS. Differential effects between intravenous and targeted renal delivery of fenoldopam on renal function and blood pressure in patients undergoing cardiac catheterization. The American Journal of Cardiology. 2006;97(7):1076–1081. doi: 10.1016/j.amjcard.2005.10.053. [DOI] [PubMed] [Google Scholar]
- 37.Kurnik BRC, Allgren RL, Center FC, Solomon RJ, Bates ER, Weisberg LS. Prospective study of atrial natriuretic peptide for the prevention of radiocontrast-induced nephropathy. The American Journal of Kidney Diseases. 1998;31(4):674–680. doi: 10.1053/ajkd.1998.v31.pm9531185. [DOI] [PubMed] [Google Scholar]
- 38.Wang A, Holcslaw T, Bashore TM, et al. Exacerbation of radiocontrast nephrotoxicity by endothelin receptor antagonism. Kidney International. 2000;57(4):1675–1680. doi: 10.1046/j.1523-1755.2000.00012.x. [DOI] [PubMed] [Google Scholar]
- 39.Koch J-A, Plum J, Grabensee B, Mödder U. Prostaglandin E1: a new agent for the prevention of renal dysfunction in high risk patients caused by radiocontrast media? Nephrology Dialysis Transplantation. 2000;15(1):43–49. doi: 10.1093/ndt/15.1.43. [DOI] [PubMed] [Google Scholar]
- 40.Russo D, Minutolo R, Cianciaruso B, Memoli B, Conte G, de Nicola L. Early effects of contrast media on renal hemodynamics and tubular function in chronic renal failure. Journal of the American Society of Nephrology. 1995;6(5):1451–1458. doi: 10.1681/ASN.V651451. [DOI] [PubMed] [Google Scholar]
- 41.Miller HI, Dascalu A, Rassin TA, Wollman Y, Chernichowsky T, Iaina A. Effects of an acute dose of L-Arginine during coronary angiography in patients with chronic renal failure: a randomized, parallel, double-blind clinical trial. The American Journal of Nephrology. 2003;23(2):91–95. doi: 10.1159/000068036. [DOI] [PubMed] [Google Scholar]
- 42.Sporer H, Lang F, Oberleithner H. Inefficacy of bicarbonate infusions on the course of postischaemic acute renal failure in the rat. European Journal of Clinical Investigation. 1981;11(4):311–315. doi: 10.1111/j.1365-2362.1981.tb02122.x. [DOI] [PubMed] [Google Scholar]
- 43.Merten GJ, Burgess WP, Gray LV, et al. Prevention of contrast-induced nephropathy with sodium bicarbonate: a randomized controlled trial. Journal of the American Medical Association. 2004;291(19):2328–2334. doi: 10.1001/jama.291.19.2328. [DOI] [PubMed] [Google Scholar]
- 44.Brar SS, Shen AY-J, Jorgensen MB, et al. Sodium bicarbonate vs sodium chloride for the prevention of contrast medium-induced nephropathy in patients undergoing coronary angiography: a randomized trial. Journal of the American Medical Association. 2008;300(9):1038–1046. doi: 10.1001/jama.300.9.1038. [DOI] [PubMed] [Google Scholar]
- 45.Maioli M, Toso A, Leoncini M, et al. Sodium bicarbonate versus saline fort he prevention of contrast-induced nephropathy in patients with renal dysfunction undergoing coronary angiography or intervention. Journal of the American College of Cardiology. 2008;52(8):599–604. doi: 10.1016/j.jacc.2008.05.026. [DOI] [PubMed] [Google Scholar]
- 46.Brar SS, Hiremath S, Dangas G, Mehran R, Brar SK, Leon MB. Sodium bicarbonate for the prevention of contrast induced-acute kidney injury: a systematic review and meta-analysis. Clinical Journal of the American Society of Nephrology. 2009;4(10):1584–1592. doi: 10.2215/CJN.03120509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hiremath S, Brar SS. The evidence for sodium bicarbonate therapy for contrast-associated acute kidney injury: far from settled science. Nephrology Dialysis Transplantation. 2010;25(8):2802–2804. doi: 10.1093/ndt/gfq279. [DOI] [PubMed] [Google Scholar]
- 48.Hoste EAJ, De Waele JJ, Gevaert SA, Uchino S, Kellum JA. Sodium bicarbonate for prevention of contrast-induced acute kidney injury: a systematic review and meta-analysis. Nephrology Dialysis Transplantation. 2010;25(3):747–758. doi: 10.1093/ndt/gfp389. [DOI] [PubMed] [Google Scholar]
- 49.Meier P, Ko DT, Tamura A, Tamhane U, Gurm HS. Sodium bicarbonate-based hydration prevents contrast-induced nephropathy: a meta-analysis. BMC Medicine. 2009;7, article 23 doi: 10.1186/1741-7015-7-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Zoungas S, Ninomiya T, Huxley R, et al. Systematic review: sodium bicarbonate treatment regimens for the prevention of contrast-induced nephropathy. Annals of Internal Medicine. 2009;151(9):631–638. doi: 10.7326/0003-4819-151-9-200911030-00008. [DOI] [PubMed] [Google Scholar]
- 51.Tepel M, Van Der Giet M, Schwarzfeld C, Laufer U, Liermann D, Zidek W. Prevention of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. The New England Journal of Medicine. 2000;343(3):180–184. doi: 10.1056/NEJM200007203430304. [DOI] [PubMed] [Google Scholar]
- 52.Berwanger O. Acetylcysteine for prevention of renal outcomes in patients undergoing coronary and peripheral vascular angiography: main results from the randomized acetylcysteine for contrast-induced nephropathy trial (ACT) Circulation. 2011;124(11):1250–1259. doi: 10.1161/CIRCULATIONAHA.111.038943. [DOI] [PubMed] [Google Scholar]
- 53.Nallamothu BK, Shojania KG, Saint S, et al. Is acetylcysteine effective in preventing contrast-related nephropathy? A meta-analysis. The American Journal of Medicine. 2004;117(12):938–947. doi: 10.1016/j.amjmed.2004.06.046. [DOI] [PubMed] [Google Scholar]
- 54.Bagshaw SM, Ghali WA. Acetylcysteine for prevention of contrast-induced nephropathy after intravascular angiography: a systematic reveiw and meta-analysis. BMC Medicine. 2004;2 doi: 10.1186/1741-7015-2-38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gonzales DA, Norsworthy KJ, Kern SJ, et al. A meta-analysis of N-acetylcysteine in contrast-induced nephrotoxicity: unsupervised clustering to resolve heterogeneity. BMC Medicine. 2007;5, article 32 doi: 10.1186/1741-7015-5-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Sun Z, Fu Q, Cao L, et al. Intravenous N-acetylcysteine for prevention of contrast-induced nephropathy: a meta-analysis of randomized controlled trials. PLoS ONE. 2013;8 doi: 10.1371/journal.pone.0055124.e55124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Briguori C, Colombo A, Violante A, et al. Standard vs double dose of N-acetylcysteine to prevent contrast agent associated nephrotoxicity. European Heart Journal. 2004;25(3):206–211. doi: 10.1016/j.ehj.2003.11.016. [DOI] [PubMed] [Google Scholar]
- 58.Baker CSR, Wragg A, Kumar S, De Palma R, Baker LRI, Knight CJ. A rapid protocol for the prevention of contrast-induced renal dysfunction: the RAPPID study. Journal of the American College of Cardiology. 2003;41(12):2114–2118. doi: 10.1016/s0735-1097(03)00487-x. [DOI] [PubMed] [Google Scholar]
- 59.Ludwig U, Riedel MK, Backes M, Imhof A, Muche R, Keller F. MESNA (sodium 2-mercaptoethanesulfonate) for prevention of contrast medium-induced nephrotoxicity—controlled trial. Clinical Nephrology. 2011;75(4):302–308. doi: 10.5414/cn106651. [DOI] [PubMed] [Google Scholar]
- 60.Bagshaw SM, Ghali WA. Theophylline for prevention of contrast-induced nephropathy: a systematic review and meta-analysis. Archives of Internal Medicine. 2005;165(10):1087–1093. doi: 10.1001/archinte.165.10.1087. [DOI] [PubMed] [Google Scholar]
- 61.Kabasakal L, Şehirli AÖ, Çetinel Ş, Cikler E, Gedik N, Şener G. Mesna (2-mercaptoethane sulfonate) prevents ischemia/reperfusion induced renal oxidative damage in rats. Life Sciences. 2004;75(19):2329–2340. doi: 10.1016/j.lfs.2004.04.029. [DOI] [PubMed] [Google Scholar]
- 62.Spargias K, Alexopoulos E, Kyrzopoulos S, et al. Ascorbic acid prevents contrast-mediated nephropathy in patients with renal dysfunction undergoing coronary angiography or intervention. Circulation. 2004;110(18):2837–2842. doi: 10.1161/01.CIR.0000146396.19081.73. [DOI] [PubMed] [Google Scholar]
- 63.Sadat U, Usmann A, Gillard JH, Boyle JR. Does ascorbic acid protect against contrast-induced acute kidney injury in patients undergoing coronary angiography: a systematic review with meta-analysis of randomized, controlled trials. Journal of the American College of Cardiology. 2013;62:2167–2175. doi: 10.1016/j.jacc.2013.07.065. [DOI] [PubMed] [Google Scholar]
- 64.Khanal S, Attallah N, Smith DE, et al. Statin therapy reduces contrast-induced nephropathy: an analysis of contemporary percutaneous interventions. The American Journal of Medicine. 2005;118(8):843–849. doi: 10.1016/j.amjmed.2005.03.031. [DOI] [PubMed] [Google Scholar]
- 65.Patti G, Nusca A, Chello M, et al. Usefulness of statin pretreatment to prevent contrast-induced nephropathy and to improve long-term outcome in patients undergoing percutaneous coronary intervention. The American Journal of Cardiology. 2008;101(3):279–285. doi: 10.1016/j.amjcard.2007.08.030. [DOI] [PubMed] [Google Scholar]
- 66.Jo SH, Koo BK, Park JS, et al. Prevention of radiocontrast medium-induced nephropathy using short-term high-dose simvastatin in patients with renal insufficiency undergoing coronary angiography (PROMISS) trial-a randomized controlled study. The American Heart Journal. 2008;155(3):499.e1–499.e8. doi: 10.1016/j.ahj.2007.11.042. [DOI] [PubMed] [Google Scholar]
- 67.Toso A, Maioli M, Leoncini M, et al. Usefulness of atorvastatin (80mg) in prevention of contrast-induced nephropathy in patients with chronic renal disease. The American Journal of Cardiology. 2010;105(3):288–292. doi: 10.1016/j.amjcard.2009.09.026. [DOI] [PubMed] [Google Scholar]
- 68.Patti G, Ricottini E, Nusca A, et al. Short-term, high-dose atorvastatin pretreatment to prevent contrast-induced nephropathy in patients with acute coronary syndromes undergoing percutaneous coronary intervention (from the ARMYDA-CIN [atorvastatin for reduction of myocardial damage during angioplasty-contrast-induced nephropathy] trial. The American Journal of Cardiology. 2011;108(1):1–7. doi: 10.1016/j.amjcard.2011.03.001. [DOI] [PubMed] [Google Scholar]
- 69.Quintavalle C, Fiore D, De Micco F, et al. Impact of high loading dose of atorvastatin on contrast-induced acute kidney injury. Circulation. 2012;126:3008–3016. doi: 10.1161/CIRCULATIONAHA.112.103317. [DOI] [PubMed] [Google Scholar]
- 70.Moscucci M. Contrast-induced acute kidney injury: the continuous quest for pharmacological prevention. Circulation: Cardiovascular Interventions. 2012;5:741–743. doi: 10.1161/CIRCINTERVENTIONS.112.976126. [DOI] [PubMed] [Google Scholar]
- 71.Leoncini M, Toso A, Maioli M, et al. Early high-dose rosuvastatin for contrast-induced nephropathy prevention in acute coronary syndrom: results from the PRATO-ACS study (protective effect of rosuvastatin and antiplatelet therapy on contrast-induced acute kidney injury and myocardial damage in patients with acute coronary syndrome) Journal of the American College of Cardiology. 2014;63:71–79. doi: 10.1016/j.jacc.2013.04.105. [DOI] [PubMed] [Google Scholar]
- 72.Frank H, Werner D, Lorusso V, et al. Simultaneous hemodialysis during coronary angiography fails to prevent radiocontrast-induced nephropathy in chronic renal failure. Clinical Nephrology. 2003;60(3):176–182. doi: 10.5414/cnp60176. [DOI] [PubMed] [Google Scholar]
- 73.Vogt B, Ferrari P, Schönholzer C, et al. Prophylactic hemodialysis after radiocontrast media in patients with renal insufficiency is potentially harmful. The American Journal of Medicine. 2001;111(9):692–698. doi: 10.1016/s0002-9343(01)00983-4. [DOI] [PubMed] [Google Scholar]
- 74.Lehnert T, Keller E, Gondolf K, Schäffner T, Pavenstädt H, Schollmeyer P. Effect of haemodialysis after contrast medium administration in patients with renal insufficiency. Nephrology Dialysis Transplantation. 1998;13(2):358–362. doi: 10.1093/oxfordjournals.ndt.a027830. [DOI] [PubMed] [Google Scholar]
- 75.Moon SS, Back S-E, Kurkus J, Nilsson-Ehle P. Hemodialysis for elimination of the nonionic contrast medium lohexol after angiography in patients with impaired renal function. Nephron. 1995;70(4):430–437. doi: 10.1159/000188641. [DOI] [PubMed] [Google Scholar]
- 76.Marenzi G, Marana I, Lauri G, et al. The prevention of radiocontrast-agent-induced nephropathy by hemofiltration. The New England Journal of Medicine. 2003;349(14):1333–1340. doi: 10.1056/NEJMoa023204. [DOI] [PubMed] [Google Scholar]
- 77.Marenzi G, Lauri G, Campodonico J, et al. Comparison of two hemofiltration protocols for prevention of contrast-induced nephropathy in high-risk patients. The American Journal of Medicine. 2006;119(2):155–162. doi: 10.1016/j.amjmed.2005.08.002. [DOI] [PubMed] [Google Scholar]
- 78.Barrett BJ, Carlisle EJ. Metaanalysis of the relative nephrotoxicity of high- and low-osmolality iodinated contrast media. Radiology. 1993;188(1):171–178. doi: 10.1148/radiology.188.1.8511292. [DOI] [PubMed] [Google Scholar]
- 79.From AM, Al Badarin FJ, McDonald FS, Bartholmai BJ, Cha SS, Rihal CS. Iodixanol versus low-osmolar contrast media for prevention of contrast induced nephropathy meta-analysis of randomized, controlled trials. Circulation: Cardiovascular Interventions. 2010;3(4):351–358. doi: 10.1161/CIRCINTERVENTIONS.109.917070. [DOI] [PubMed] [Google Scholar]
- 80.Stacul F, van der Molen AJ, Reimer P, et al. Contrast induced nephropathy: updated ESUR Contrast Media Safety Committee guidelines. European Radiology. 2011;21(12):2527–2541. doi: 10.1007/s00330-011-2225-0. [DOI] [PubMed] [Google Scholar]