
Figure 2.
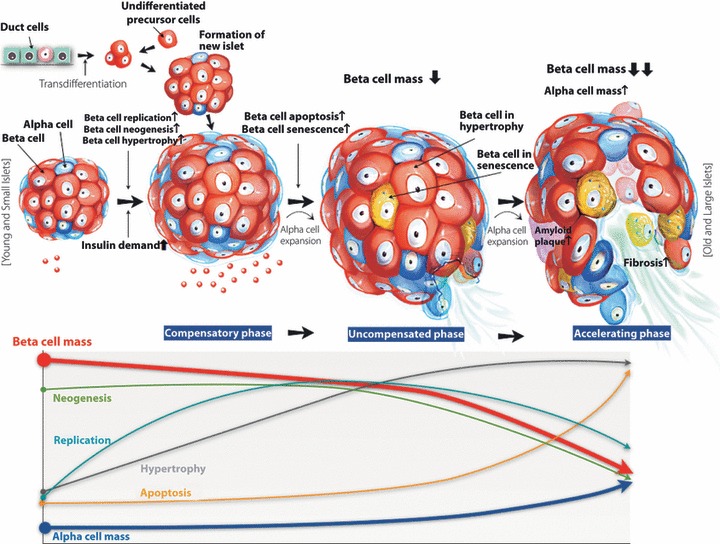
Hypothesis for morphological alterations of islets and β‐cell reductions in diabetic patients. Factors that increase insulin resistance, such as obesity, increased calorie intake and decreased physical activity, could stimulate an increase in β‐cell mass through β‐cell replication, β‐cell neogenesis or β‐cell hypertorphy, maintaining a compensatory phase and normoglycemia. However, a sustained increase in insulin demand could cause β‐cell apoptosis through glucose toxicity, lipid toxicity, and chronic inflammation and increased oxidative stress resulting in an uncompensated phase with reduced β‐cell mass and hyperglycemia. Genetic background or intrauterine nutrition could limit β‐cell expansion. Pharmacological agents, such as sulfonylurea, could play a role to increase β‐cell apoptosis. An uncompensated phase could progress to an accelerating phase with severe β‐cell loss over time through increased fibrosis and amyloidosis, as well as increased β‐cell toxicity as described earlier. Furthermore, an increase in α‐cell mass could aggravate hyperglycemia. Finally, the decline in β‐cell mass caused by apoptosis and increased α‐cell mass could aggravate hyperglycemia in diabetic subjects over time.