
Figure 2.
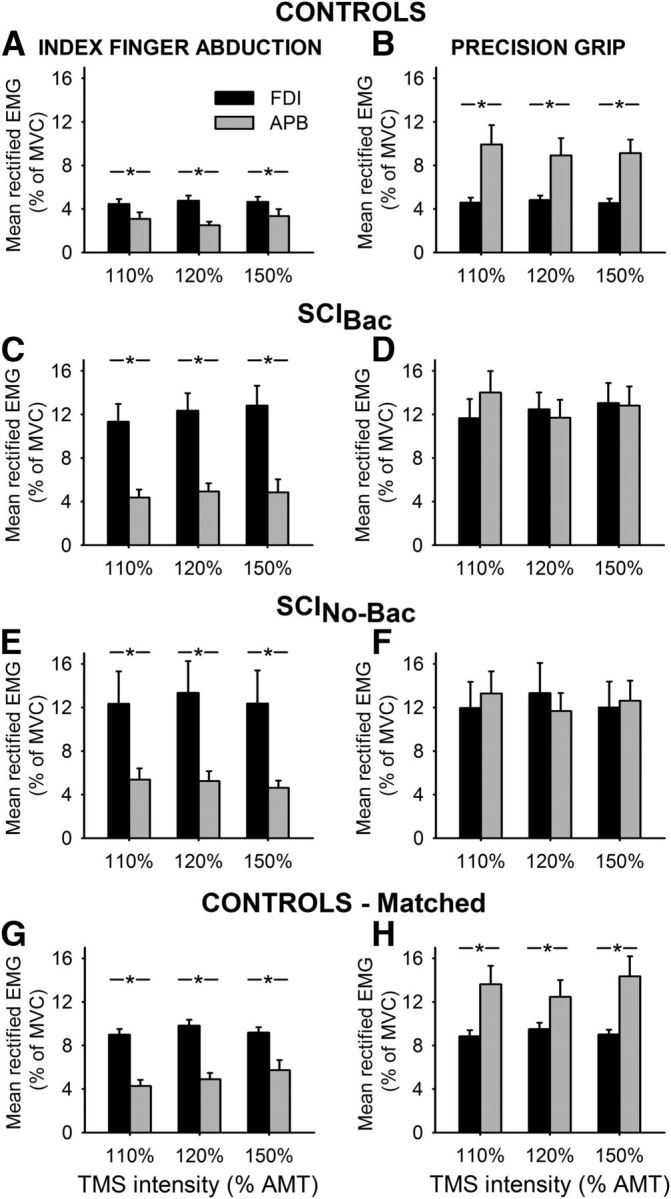
EMG recordings. Group data show the mean rectified EMG activity in the FDI (black bars) and APB (gray bars) in healthy controls (A, B, n = 15), SCI patients taking baclofen (C, D, SCIBac, n = 10) and in patients who never took baclofen (E, F, SCINo-Bac, n = 11) during index finger abduction (left column) and precision grip (right column). Note that we included 12 participants in the SCIBac group and 10 of them participated in most measurements. The additional 2 patients were included only for the svEMG test. Mean rectified EMG activity in both muscles was obtained 100 ms before TMS stimulus artifact during testing of MEPs at increasing TMS intensities. The abscissa shows the TMS stimulus intensity used during testing (110%, 120%, and 150% of AMT). The ordinate shows the mean rectified EMG activity as a percentage of the MVC in each muscle tested. Note that EMG activity in the FDI muscle was matched during index finger abduction and precision grip in all groups. Also note that the EMG strategy used by controls and patients during precision grip was different. Here, control subjects activated the APB to a larger extent than the FDI muscle, whereas both groups of patients activated both muscles to a similar extent. Additional testing showed that control subjects were able to increase EMG activity to match EMG levels in patients during both tasks (G, H; controls matched, n = 11). Error bars indicate SE. *p < 0.05.