
Fig. 2.
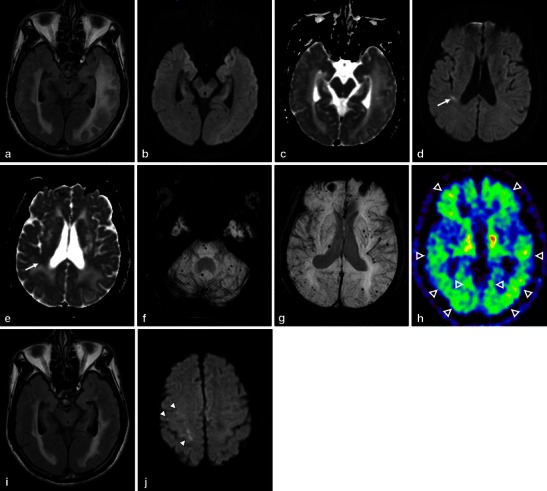
CAA-related inflammation, MBs, and microinfarctions in a 72-year-old man. An axial FLAIR image (a) showed large confluent asymmetric hyperintense lesions, which involved not only the left dominant subcortical white matter but also the overlying left temporo-occipital cortices, with a mass effect. Low signal intensity on DWI (b) and increased diffusion on the ADC map (c) suggested vasogenic oedema. In addition to these white matter lesions, DWI (d) demonstrated a small right temporal hyperintense lesion (arrow) with corresponding decreased diffusion (arrow) on the ADC map (e) (arrow). This signal change indicated a relatively acute microinfarction. An axial 3D T2*-weighted image (f, g) revealed multiple MBs, which were distributed not only in the posterior dominant cortical-subcortical region but also in the left putamen, right thalamus, pons and cerebellum. A PiB-PET image (h) revealed the diffuse cortical accumulation, including the occipital lobes, higher than those of the cerebral white matter, which indicated the global PiB uptake (open arrowheads). These finding of MBs and PiB distribution suggested the coexistence of CAA and hypertensive arteriopathy. Two months after a course of intravenous steroid therapy, an improvement in the white matter lesions was identified on a FLAIR image (i). However, DWI (j) revealed new subcortical microinfarctions in the right frontal lobe (arrowheads)