

Abstract
Background
There is a general belief that gastro-oesophageal reflux increases after meals and especially following a rapid intake.
Objective
To evaluate the impact of rapid vs. slow food intake on gastro-oesophageal reflux disease (GORD) patients.
Materials and methods
Forty-six GORD patients with heartburn and / or acid regurgitation once a week or more often common were included in this study. Participants were asked to eat the same standard meal within either 5 or 30 minutes under observation in a random order on 2 consecutive days. A total of 28 hours of recording were obtained by intraoesophageal impedance pH and number of liquid and mixed reflux episodes within 3 hours of the slow- and fast-eating postprandial periods were calculated.
Results
While all patients defined GORD symptoms, 10 (21.7%) had pathological 24-h intraoesophageal impedance measurement, 15 (32.6%) had pathological DeMeester and 21.7% had erosive oesophagitis. No difference has been shown according to the eating speed when all reflux episodes were taken together (754 vs. 733). Speed of food intake also did not have an impact on patients with normal vs. pathological 24-h intraoesophageal impedance or erosive vs. non-erosive. During the first postprandial hour, approximately half of the reflux events were non-acid, compared to 34.2% during the second hour and 26.8% during the third hour (p < 0.001). The number of acid reflux episodes was significantly higher than non-acid reflux especially during the second and third hours and in total for 3 hours.
Conclusions
This first study addressing the effect of eating speed on reflux episodes in GORD patients did not support the general belief that reflux increases following fast eating. Acid and non-acid reflux were similar at the first postprandial hour, then acid reflux episodes were predominantly higher, which implicate the importance of acid pockets.
Keywords: Eating, food habits, gastro-oesophageal reflux, MII, oesophageal pH monitoring, proton-pump inhibitors
Introduction
Many factors contribute to an increase in postprandial gastro-oesophageal reflux (GOR). Some dietary factors, smoking cigarettes, and drinking alcohol may trigger reflux symptoms, and it is generally recommended that they should be avoided. Moreover, lifestyle changes, such as eating before bedtime, head elevation after meals, activity, obesity, and the timing and size of the meal may also exacerbate symptoms. GOR usually increases after meals, and there is a general belief that the speed of eating may influence reflux symptoms.1–8 In a study in which patients self-reported their experiences of the causes of reflux, patients stated that dietary factors, including eating speed, triggered reflux symptoms.9 However, this was a questionnaire-based study, and the effect of the speed of eating on reflux was not investigated with an objective methodology, such as intraoesophageal ambulatory impedance-pH monitoring (MII). The effect of rapid food intake on GORD has been investigated in healthy volunteers, and the results showed that reflux increased after meals, especially during the first postprandial hour. The dominant nature of the reflux was non-acid reflux.8 However, this study was performed in healthy volunteers, and it has been shown that non-acid reflux increases in healthy controls, while acid reflux has been shown to dominate in patients with GORD.10 We previously used 24-hour intraoesophageal pH monitoring to show that slow eating increases the number of acid reflux events.11 Because 24-hour intraoesophageal pH monitoring only measures refluxes that are acid, we performed the present study using multichannel intraluminal impedance-pH to determine the impact of rapid vs. slow food intake on GORD patients. The aim of this study is to investigate the effect of eating speed on gastro-oesophageal reflux episodes and to determine a scientific basis for recommendations concerning the eating speed of patients with reflux.
Materials and methods
Patients
The study was conducted at Ege University School of Medicine in the Reflux Outpatient Clinic and was approved by Ege University Ethics Committee (08.12.2009/09-5.1/3). Patients over 18 years old with heartburn and/or regurgitation once a week or more often who were referred for 24-h intraoesophageal MII-pH monitoring were evaluated. Upper gastrointestinal endoscopy was performed in all patients. Patients with gastric outlet obstructions, gastroparesis, medications affecting gastrointestinal motility, malabsorption, upper gastrointestinal surgery, any cancer except non-melanoma skin cancers, pregnancy, eating disorders, hiatal hernia larger than 3 cm, systemic disorders such as uncontrolled diabetes, renal failure, cerebrovascular disease, major psychiatric disease, alcoholism, drug abuse, peptic ulcers, Zollinger Ellison syndrome, primary oesophageal motility disorders, inflammatory bowel disease, or cirrhosis of the liver and patients who refused to participate were excluded from the study.
Study design
Proton-pump inhibitors, H2 blockers, and antacids were stopped 7 days before the procedure. Abstinence from eating for at least 6 hours was required before the procedure. An oesophageal manometry with a water-perfused 8-channel motility catheter was performed to determine the upper margin of the lower oesophageal sphincter before placing the MII-pH catheter and to rule out any oesophageal motility problems. After determining the location of the lower oesophageal sphincter (LOS), a MII-pH catheter (MMS Greenfield pH-MII catheter) was placed 5 cm proximally to the LOS and connected to the ambulatory recorder (MMS Ohmega, The Netherlands) and about 28 h of pH-MII was measured in all patients including two eating periods for the study (Figure 1). After the placing of the catheter following a stabilization period for 1 hour, patients were asked to eat the same standard meal (a double cheeseburger, 1 banana, 100 g yoghurt, and 200 ml water) within either 5 or 30 minutes in a random order on two consecutive days. The timing of the postprandial period immediately began with the completion of the meal. Eating period was started on the same time at the following day. The caloric content of the standard meal was 744 kcal (41.2% fat, 37.6% carbohydrate, 21.2% protein). Patients did not drink or eat any other food during the 3-h period after the meal. All patients were observed to determine whether they were able to eat during the specified time, and the time of completion was recorded by the observer. The patients were also asked to sit in an upright position after the meal for 3 hours. The catheter was removed at the end of the 3 hours after the second day’s meal.
Figure 1.
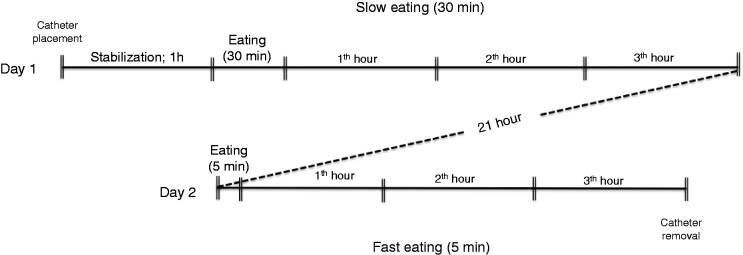
Study design.
The same standard meal was eaten within either 5 or 30 minutes in a random order on two consecutive days. Eating period was started on the same time at the following day. Total measurement period was about 28 hours.
Analysis
The data were transferred to a computer and 3 hours of MII-pH tracings were analysed not only by the software but also manually by a blinded investigator. Liquid and mixed episodes were calculated. Gas-only reflux events were not evaluated. Acid reflux was defined as a reflux episode in which the oesophageal pH fell below 4 for at least 20 seconds or as reflux that occurs when the oesophageal pH was already below 4. Non-acid reflux was defined as pH ≥4.
Statistics
Statistical analyses were performed using SPSS for Windows 11.0 (SPSS, Chicago, IL, USA). After conducting the descriptive statistics, statistical comparisons were performed using Student’s t-test and chi-squared test. p-values < 0.05 were considered to be statistically significant.
Results
Forty-six GORD patients with heartburn and/or regurgitation at least once per week were included in this study. Thirty-two (69.6%) of the patients were female and the median was 43 ± 10 years (18–68 years). Upper gastrointestinal endoscopy revealed that 10 (21.7%) patients had erosive oesophagitis (five with LA-A and five with LA-B) and 36 had normal oesophagus. No Barrett oesophagus was diagnosed. pH-MII studies showed that 10 (21.7%) patients had pathological 24-h intraoesophageal impedance measurement and 15 (32.6%) had pathological DeMeester. Number of reflux episodes (acid and non-acid) following 3 hours of slow- and fast-eating postprandial periods were evaluated for the study. A total of 1487 reflux episodes were detected in 92 studies during the entire two times of the 3-h postprandial period, 885 of which were acid and 602 of which were non-acid.
In the fast-eating group, a total of 46 GORD patients yielded a total of 754 reflux episodes over a 3-h postprandial period, of which 474 were acid and 279 were non-acid. In the slow-eating group, 46 GORD patients yielded a total of 733 reflux episodes, of which 410 were acid and 323 were non-acid.
There was no statistically significant difference at the first, second, and third postprandial hours and total 3 hours between fast and slow-eating groups regarding either the number of acid or non- acid reflux episodes (Table 1). Ten (21.7%) patients with pathological 24-h intraoesophageal impedance measurement were also compared to normal 24-h measurement according to the eating speed for 3 hours and both number of acid and non-acid reflux episodes and the results were not significantly different. Similar to these findings, when patients were divided according to endoscopic findings, no difference was detected between erosive (n = 10) and non-erosive reflux disease (n = 36) groups related with the speed of food intake. Irrespective of the speed of eating, number of acid reflux episodes was stable within the first 2 hours following a meal, after which dropped slightly. When slow- and fast-eating acid episodes were evaluated together, there was no difference between first and second hours (323 vs. 324, p = 0.97); however, number of episodes at first (323 vs. 237, p = 0.005) and second (324 vs. 237, p = 0.0004) hours was significantly higher than at third hour. However, number of non-acid reflux episodes was as high as the acid reflux in the first hour (347 vs. 323, p = 0.71) and then decreased significantly compared to acid reflux episodes at second (168 vs. 324, p = 0.002), third (87 vs. 237, p = 0.00002), and total 3 hours (602 vs. 884, p = 0.03). When slow and fast-eating non-acid episodes were evaluated together, the number of episodes were higher at the first vs. second hour (347 vs. 168, p = 0.0001), and likewise higher at first vs. third hour (347 vs. 87, p = 0.000005) (Figure 2).
Table 1.
Number of reflux episodes within 3 hours of the study period in 46 patients
| Postprandial hours | Fast eating (5 min) |
Slow eating (30 min) |
||||
|---|---|---|---|---|---|---|
| Non-acid | Acid | Total | Non-acid | Acid | Total | |
| 1st | 161 (48.8) | 169 (51.2) | 330 (100) | 186 (54.7) | 154 (45.3) | 340 (100) |
| 2nd | 72 (28.8) | 178 (71.2) | 250 (100) | 96 (39.7) | 146 (60.3) | 242 (100) |
| 3rd | 46 (26.6) | 127 (73.4) | 173 (100) | 41 (27.2) | 110 (72.8) | 151 (100) |
| Total | 279 (37.0) | 474 (63.0) | 753 (100) | 323 (44.1) | 410 (55.9) | 733 (100) |
Values are n (%). No difference was shown with the speed of food intake.
Figure 2.
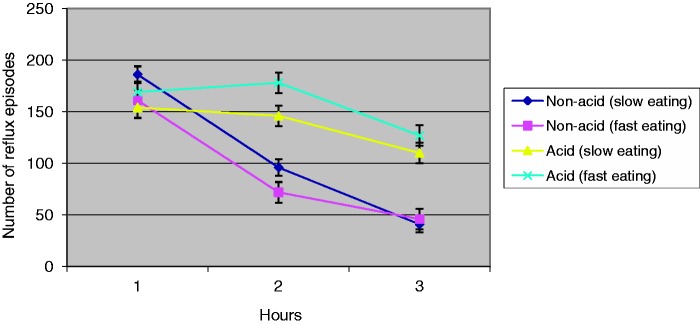
Number of acid and non-acid reflux episodes for the slow- and fast-eating periods following intake of standard meal.
Discussion
We evaluated the effect of eating speed on gastro-oesophageal reflux episodes in patients with GORD symptoms. No difference has been shown between rapid and slow intake when all reflux episodes evaluated together. Acid reflux episodes were equal to non-acid during the first postprandial hour (48.2%) and increased at second (65.8%) and third hour (73.1%). All patients defined GORD symptoms once a week or common; however, 10 (21.7%) had pathological 24-h intraoesophageal impedance measurement and again no difference was shown between patients with normal or pathological 24-h measurement for rapid or slow intake of food. Our data indicates that eating speed does not have any impact on reflux episodes.
In our previous study, we compared the effect of fast food intake vs. slow food intake on reflux episodes using pH-monitoring in patients with GOR. No significant difference was shown between the parameters (number of refluxes, time of reflux episodes, number of symptoms, primarily heartburn or acid regurgitation) obtained in the fast-eating period compared to the slow-eating period.11
The only study addressing the effect of eating speed was performed by Wildi et al.8 with an intraoesophageal MII in 20 healthy volunteers. Their study protocol was similar to the protocol used in the present study except for the time frame, which was 2 hours after meals and the number of volunteers. They revealed that fast eating (within 5 min) was associated with more reflux compared with slow eating (within 30 min), especially in the first hour, and that reflux episodes were primarily correlated with non-acid reflux. These results were different from the results in our GORD patients, as our results showed predominantly acid reflux.
Studies show that factors contributing to reflux are multifactorial and that one factor alone is not responsible for reflux. Recently, an acid pocket was described as postprandial highly acidic unbuffered gastric juice at the gastro-oesophageal junction.12–14 This phenomenon is particularly important because postprandial exposure of the distal oesophagus to acid has been implicated in lesions in the distal oesophagus. In a study by Kwiatek et al.,15 patients with GORD were studied fasted, 20 minutes after a high-fat diet, and 20 minutes after an alginate-antacid combination. An acid pocket was displaced distant from the proximal stomach and the gastro-oesophageal junction in patients with acidic segments placed at the proximal stomach in the fasted and postprandial period. Although we did not evaluate the acid pocket in our study, we showed that refluxes are predominantly acid in nature, lasting 3 hours, and it is possible that an acid pocket or acid that has not mixed homogeneously with a meal may play a primary role in reflux in the postprandial period.
Increased transient lower oesophageal sphincter relaxations (TLOSRs) may also play a role in postprandial reflux events. Sifrim et al.10 studied MII pH monitoring in patients with GORD and in controls. TLOSRs were equally frequent in each group. GOR patients experienced more acid reflux, whereas the control group experienced more non-acid reflux. This finding may explain the differences between the study by Wildi et al.8 and our study. Scheffer et al.16 evaluated the effect of proximal gastric distention on TLOSRs and found an increase in TLOSRs in healthy people. Especially, it might be expected the fast eating could lead to more rapid and possibly greater distension of the proximal stomach, at least in the first hour. Our study did not aim to measure whether this phenomenon is responsible about the predominantly acid reflux following eating. However, since no difference was observed between groups according to the eating speed, it might be speculated that a distended stomach does not play an important role.
We conclude that no difference has been shown according to the eating speed when all reflux episodes were evaluated together in patients with normal or pathological 24-h intraoesophageal impedance or patients with/without erosive oesophagitis. However, acid reflux was the major reflux phenomenon especially at second and third hours following food intake. Especially acid pocket and incomplete proximal stomach relaxation with different acid mixtures of food may explain our findings.
This first study addressing the effect of eating speed on reflux episodes in GORD patients suggests that the general belief about the suggestion to the patients to eat slowly possibly is not a necessary behavioural modification.
Funding
This study was supported by Ege reflux study group, grant number: 08.12.2009/09-5.1/3.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- 1.Salvia G, De Vizia B, Manguso F, et al. Effect of intragastric volume and osmolality on mechanisms of gastroesophageal reflux in children with gastroesophageal reflux disease. Am J Gastroenterol 2001; 96: 1725–1732 [DOI] [PubMed] [Google Scholar]
- 2.Nowak M, Büttner P, Harrison S, et al. Effectiveness of lifestyle measures in the treatment of gastroesophageal reflux disease – a case series. Ther Clin Risk Manag 2006; 2: 329–334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.El-Serag HB, Satia JA, Rabeneck L. Dietary intake and the risk of gastrooesophageal reflux disease: a cross sectional study in volunteers. Gut 2005; 54: 11–17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Murphy DW, Castell DO. Chocolate and heartburn: evidence of increased esophageal acid exposure after chocolate ingestion. Am J Gastroenterol 1988; 83: 633–636 [PubMed] [Google Scholar]
- 5.Becker DJ, Sinclair J, Castell DO, et al. A comparison of high and low fat meals on postprandial esophageal acid exposure. Am J Gastroenterol 1989; 84: 782–786 [PubMed] [Google Scholar]
- 6.Nebel OT, Castell DO. Inhibition of the lower oesophageal sphincter by fat – a mechanism for fatty food intolerance. Gut 1973; 14: 270–274 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Schönfeld J, Evans DF. Fat, spices and gastro-oesophageal reflux. Z Gastroenterol 2007; 45: 171–175 [DOI] [PubMed] [Google Scholar]
- 8.Wildi SM, Tutuian R, Castell DO. The influence of rapid food intake on postprandial reflux: studies in healthy volunteers. Am J Gastroenterol 2004; 99: 1645–1651 [DOI] [PubMed] [Google Scholar]
- 9.Dibley LB, Norton C, Jones R. Don't eat tomatoes: patient's self-reported experiences of causes of symptoms in gastro-oesophageal reflux disease. Fam Pract 2010; 27: 410–417 [DOI] [PubMed] [Google Scholar]
- 10.Sifrim D, Holloway R, Silny J, et al. Composition of the postprandial refluxate in patients with gastroesophageal reflux disease. Am J Gastroenterol 2001; 96: 647–655 [DOI] [PubMed] [Google Scholar]
- 11. Valitova ER, Bayrakci B and Bor S. The effect of the speed of eating on acid reflux and symptoms of patients with gastroesophageal reflux disease. Turkish J Gastroenterol (in press) [PubMed]
- 12.Boeckxstaens GE. Alterations confined to the gastrooesophageal junction: the relationship between low LOSP, TLOSRs, hiatus hernia and acid pocket. Best Pract Res Clin Gastroenterol 2010; 24: 821–829 [DOI] [PubMed] [Google Scholar]
- 13.Beaumont H, Bennink RJ, de Jong J, et al. The position of the acid pocket as a major risk factor for acidic reflux in healthy subjects and patients with GORD. Gut 2010; 59: 441–451 [DOI] [PubMed] [Google Scholar]
- 14.Fletcher J, Wirz A, Young J, et al. Unbuffered highly acidic gastric juice exists at the gastroesophageal junction after a meal. Gastroenterology 2001; 121: 775–783 [DOI] [PubMed] [Google Scholar]
- 15.Kwiatek MA, Roman S, Fareeduddin A, et al. An alginateantacid formulation (Gaviscon Double Action Liquid) can eliminate or displace the postprandial ‘acid pocket' in symptomatic GERD patients. Aliment Pharmacol Ther 2011; 34: 59–66 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Scheffer RC, Akkermans LM, Bais JE, et al. Elicitation of transient lower oesophageal sphincter relaxations in response to gastric distension and meal ingestion. Neurogastroenterol Motil 2002; 14: 647–655 [DOI] [PubMed] [Google Scholar]