

Abstract
[Purpose] The aim of this study was to analyze stabilometry in athletes during an indoor season in order to determine whether injured athletes show different stabilometric values before injury than non-injured athletes in two different training periods (volume and pre-competition periods). [Subjects] The subjects were 51 athletes from Unicaja athletic club who trained regularly. [Methods] At the end of the preseason and volume periods, athletes were subjected to bipodal and monopodal stabilometry. In addition, all injuries happening in the periods after performing stabilometry (volume and pre-competition periods) were tracked. [Results] Variance analysis of bipodal stabilometric measurements taken at the end of the preseason period showed that athletes with higher values for the center-of-pressure spread variables suffered injuries during the volume period. The right-leg monopodal stabilometric measurements taken at the end of the volume period showed that athletes with higher values in the center-of-pressure position variables suffered injuries during the pre-competition period. [Conclusion] Athletes showing the worst values for center-of-pressure spread variables are more prone to sports injuries in the subsequent training period. In monopodal measurements, athletes with poorer mediolateral stability were more prone to injuries in the subsequent training period.
Key words: Sports injury, Athletes, Postural stability
INTRODUCTION
Postural stability is deeply linked with sports injuries, and copious evidence exists indicating that postural stability is greatly reduced by sports injuries. Back in 1965, Freeman first described stabilometric alterations in patients suffering from ankle sprain and correlated lateral instability of the ankle with a lack of postural control1). After Freeman, several authors analyzed the effects of sports injuries on postural stability of athletes and concluded that its deterioration may cause re-injury or even new injuries2, 3).
In addition to previous injuries, postural stability may be affected by changes in the level of activity, as well as by its type, intensity, and volume4,5,6), which constitute a risk of injury for athletes7). Some authors have carried out prospective assessments of athletes in order to determine how stabilometric changes can be a causal factor for injuries8). McGuine et al. assessed the first two weeks of the season for basketball players, and correctly described balance as a predictor of injuries, showing that those with higher postural sway values at the start of the season were the ones most injured in the long term9). Similar results were found by Wang et al., who established a correlation between poor mediolateral stability and suffering from ankle injuries later on10). Likewise, Trojian and McKeag showed in 2006 that the ability to maintain single-leg balance of athletes at the beginning of the preseason was a predictor of ankle sprains for the autumn season11). Also, Soderman et al. correlated all lower extremity injuries with increases in postural sway in female soccer players12).
From a physiological point of view, Murphy et al. affirmed in 2003 that the main cause of deteriorated postural stability as a risk factor is an alteration in the neuromuscular control strategy, which increases intersegmental joint forces and consequently increases the development of forces involving ligaments, tendons, and muscles13).
In spite of the findings reported by these authors, whether postural stability is a predictor of sports injuries remains unclear to date. There are also some similar studies that have not reported results supporting this. Hopper et al. analyzed single-leg stability by assessing the duration for which female netball athletes could maintain a unilateral posture; however, they did not find any correlation between postural stability and an increase of injuries14). Similar results were reported by Beynnon et al. in soccer, field hockey, and lacrosse athletes15).
Based on the controversy existing regarding postural stability as an injury predictor and the evidence of effects of training on postural stability and considering that to date, no studies have taken into account the type of training as a cause of postural stability deterioration in their prospective investigations, the aim of the present study was to analyze the stabilometry in athletes during their training stage in order to determine whether injured athletes scored differently in stabilometric tests than those who were injury-free in two different training periods.
SUBJECTS AND METHODS
This was a five-month descriptive prospective study (September–January) that was divided into two parts according to the different training periods. The first part consisted of bipodal and monopodal stabilometry tests at the end of preseason (in September, mainly general exercises) and a record of injuries suffered by the athletes during the subsequent period of training, which was volume period (in October and November, with training based on alternating general and specific high-volume, low-intensity exercises). The second part consisted of bipodal and monopodal stabilometry tests at the end of volume period and a record of injuries suffered by the athletes during the subsequent period of training, which was pre-competition period (in December and January, with an majority of specific low-volume, high intensity exercises). In order to avoid interference from previous injuries, all athletes injured during the volume period were excluded in the second part. Recording of injuries was performed by a physiotherapist specialized in sports injuries.
A total of 51 track and field athletes who were from an athletic club in the city, were 17 to 35 years old and had at least three years of experience took part in the first part of the present study, after excluding those who did not train regularly or who had been injured during the preseason period. In the second part of the study, athletes who had been injured previously were excluded in order to avoid interferences in the results. Therefore, 39 athletes between the ages of 17 and 35 participed in this part of investigation. Anthropometric and demographic data are shown in Table 1.
Table 1. Statistical description of the sample.
| First part of the study n=51 |
Second part of the study n=39 |
||||||||
|---|---|---|---|---|---|---|---|---|---|
| Injured in volume period n=12 | Non-injured n=39 | Injured in pre-competition period n=6 | Non-injured n=33 | ||||||
| Age (years) | 23.2±8.0 | 22.3±7.5 | 26.5±9.0 | 21.6±7.0 | |||||
| Height (m) | 1.74±0.07 | 1.74±0.08 | 1.75±0.05 | 1.74±0.09 | |||||
| Weight (kg) | 61.0±11.0 | 62.9±11.7 | 61.5±7.9 | 63.2±12.4 | |||||
| BMI (kg/m2) | 20.1±2.4 | 20.7±2.5 | 20.1±1.5 | 20.8±2.7 | |||||
| Gender | Men | 8 | 66.7% | 27 | 69.2% | 5 | 83.3% | 22 | 66.7% |
| Women | 4 | 33.3% | 12 | 30.8% | 1 | 16.7% | 11 | 33.3% | |
| Experience (years) | 7.8±4.7 | 7.2±4.6 | 10.0±4.8 | 6.7±4.4 | |||||
Quantitative variables are shown as means and SD. Categorical variables are shown as frequencies and percentages. p values are from the Student’s t-test and χ2 test, respectively. BMI: body mass index
Before the start of the study, all athletes were briefed on how they would be tested, and written informed consent was obtained from each subject or from their legal guardians in the case of underage athletes according to the standards of the Declaration of Helsinki (2008 revision)16). The ethics committee of the University of Jaén approved the study.
Weight and height measurements were performed with a Tefal (France) digital precision scale (100 g–300 kg) and an Asimed t201-t4 (Spain) measuring rod, respectively. For stabilometric measurements, a modular electronic baropodometer was used comprising a 120 × 160 cm Sensormédica® (Spain) platform with 19200 active sensors. The reliability of this piece of equipment has been proven in other studies17).
Athletes were subject to a bipodal and a monopodal stabilometric measurements once at the end of each period. For the bipodal test, athletes were instructed to remain as still as possible on the baropodometric platform for 52 seconds, with a between-heels separation of 5 cm and their feet forming a 30° angle. For the monopodal test, athletes stood on each of their lower limbs for 15 seconds (left leg first) at the center of the platform (Fig. 1). The following parameters were recorded for the bipodal test as well as for the left-leg and right-leg monopodal tests: length (Length) and area (Area) of the path described by the center of pressure, the speed of center of pressure movement (Speed), and the position of the center of pressure in the mediolateral (Xmean) and anteroposterior (Ymean) planes. These variables are marked with “l” or “r” to indicate whether they belong to the left or right leg, respectively. Tests were carried out before training started, in order to avoid any interference. Also, athletes were instructed not to engage in any sports activity on the day of testing.
Fig. 1.
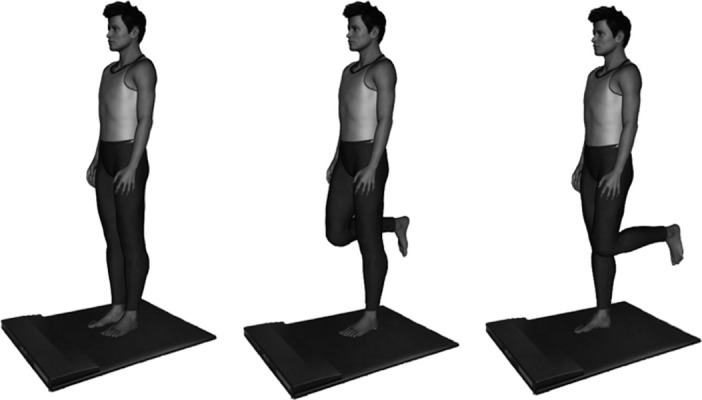
Bipodal, left monopodal and right monopodal stabilometry tests
In order to track injuries, athletes were instructed in advance and then interviewed weekly by a sports physical therapist during the volume and pre-competition periods in order to record any musculoskeletal injury on the lower limbs they might have sustained during these periods. Injury was defined as “physical damage that resulted in missing or modifying one or more training sessions or competitions” (Kolt et al., 1999)18).
A description of data included means and standard deviations for the categorical variables (Table 1). Differences in social and demographic variables between the injured and non-injured athletes each period (volume and pre-competition) were analyzed by means of the Student’s t-test for independent samples in the case of the continuous variables and a χ2 test for the categorical variables. For comparison between stabilometric variables between groups (injured and non-injured), the Student’s t-test for independent samples was used. Normality of data was assessed through a Kolmogorov-Smirnov test. These variables are underlined in tables. A significance level of p≤0.05 was set for all statistical procedures, and the SPSS v. 19 software was used.
RESULTS
Table 1 shows social and demographic statistics for the injured and non-injured subjects during the volume and pre-competition periods. There was a similar number of injured athletes in both periods. No differences were apparent in the social and demographic characteristics of the injured and non-injured athletes (p>0.05).
Table 2 shows mean values for the center-of-pressure spread and position variables in both bipodal and monopodal support at the end of the preseason period for the athletes who were injured and non-injured during the volume period. Bipodal stabilometry tests showed that those injured during the volume period had scored significantly higher in Length and Speed than those who were not injured (p=0.009 and p=0.003, respectively). Monopodal stabilometry tests did not show any statistically significant difference (p>0.05).
Table 2. Mean values of stabilometric variables in bipodal and monopodal support taken at the end of the pre-season period.
| Total injured in volume period n=12 |
Non-injured n=39 |
|||
|---|---|---|---|---|
| Preseason measures | Mean | SD | Mean | SD |
| Length (mm)* | 366.5 | 183.9 | 340.2 | 104.0 |
| Area (mm) | 36.5 | 27.1 | 47.5 | 49.9 |
| Speed (mm/sec)* | 7.4 | 3.9 | 6.7 | 2.0 |
| Xmean (mm) | 3.9 | 4.7 | 4.4 | 3.2 |
| Ymean (mm) | 4.5 | 4.1 | 6.0 | 5.1 |
| Lengthl (mm) | 272.0 | 112.5 | 267.8 | 65.5 |
| Areal (mm) | 419.1 | 493.7 | 408.7 | 350.8 |
| Speedl (mm/sec) | 24.4 | 11.4 | 24.7 | 6.8 |
| Xmeanl (mm) | 4.9 | 3.6 | 6.0 | 13.5 |
| Ymeanl (mm) | 6.6 | 5.14 | 10.2 | 8.2 |
| Lengthr (mm) | 255.6 | 119.9 | 275.5 | 82.8 |
| Arear (mm) | 340.2 | 282.9 | 378.2 | 298.8 |
| Speedr (mm/sec) | 23.1 | 12.0 | 24.7 | 7.9 |
| Xmeanr (mm) | 3.4 | 2.9 | 3.0 | 2.8 |
| Ymeanr (mm) | 7.0 | 6.5 | 8.6 | 5.2 |
Results are split for athletes injured during the volume period.
Length= Length of the path described by the center of pressure. Area=Area of the path described by the center of pressure. Speed=Speed of the center of pressure. Xmean=Mean position of the center of pressure in the mediolateral plane. Ymean=Mean position of the center of pressure in the anteroposterior plane. The first section is for bipodal support, the second section is for the left foot (indicated by addition of l to each variable), and the third section is for the right foot (indicated by addition of r to each variable). Variables underlined were normalized. *p<0.05
Table 3 displays the mean values for the center-of pressure spread and position variables in both bipodal and monopodal support at the end of the volume period for the athletes who were injured and non-injured during the pre-competition period. Right-leg monopodal stabilometry showed that injured subjects scored significantly higher with respect to Xmeanr (p=0.041). Left-leg monopodal and bipodal stabilometry did not show any statistically significant difference (p>0.05).
Table 3. Mean values of stabilometric variables in both bipodal and monopodal support at the end of the volume period.
| Total injured in pre-competition n=6 |
Non-injured n=33 |
|||
|---|---|---|---|---|
| Volume measures | Mean SD | Mean SD | ||
| Length (mm) | 310.1±131.8 | 307.7±143.6 | ||
| Area (mm) | 128.5±103.1 | 98.8±109.6 | ||
| Speed (mm/sec) | 6.2±2.8 | 13.5±42.0 | ||
| Xmean (mm) | 4.5±1.8 | 5.7±5.0 | ||
| Ymean (mm) | 8.7±2.7 | 12.4±9.4 | ||
| Lengthl (mm) | 335.3±95.9 | 316.3±127.4 | ||
| Areal (mm) | 615.0±512.0 | 489.6±506.8 | ||
| Speedl (mm/sec) | 31.1±9.6 | 35.3±40.2 | ||
| Xmeanl (mm) | 3.5±2.5 | 5.8±12.3 | ||
| Ymeanl (mm) | 10.8±7.0 | 16.3±11.6 | ||
| Lengthr (mm) | 349.0±89.3 | 322.7±132.8 | ||
| Arear (mm) | 631.1±328.3 | 608.1±624.0 | ||
| Speedr (mm/sec) | 31.9±9.4 | 36.7±40.2 | ||
| Xmeanr (mm)* | 15.2±30.3 | 4.3±3.6 | ||
| Ymeanr (mm) | 12.0±6.8 | 15.3±9.6 | ||
Results are split for athletes injured during the pre-competition period.
Length= Length of the path described by the center of pressure. Area=Area of the path described by the center of pressure. Speed=Speed of the center of pressure. Xmean=Mean position of the center of pressure in the mediolateral plane. Ymean=Mean position of the center of pressure in the anteroposterior plane. The first section is for bipodal support, the second section is for the left foot (indicated by addition of l to each variable), and the third section is for the right foot (indicated by addition of r to each variable). Variables underlined were normalized. *p<0.05
DISCUSSION
The aim of the present study was to analyze stabilometric values of athletes through their training in order to determine their value as a predictor for injuries in each of the training periods. To this end, athletes were subjected to a bipodal and monopodal stabilometry at the end of the preseason period and a tracking of their injuries in the subsequent volume period (first part). In addition, bipodal and monopodal stabilometry was carried out at the end of volume period, and tracking of their injuries was carried out in the subsequent pre-competition period (second part).
The results obtained from stabilometry at the end of the preseason period show that athletes with poorer values for center-of-pressure length and speed in bipodal support at the end of the preseason were the ones who were injured in the two subsequent months, which comprised the volume period. Although these findings agree with previous studies in which high variation of postural sway correlated or predicted posterior sports injuries9, 10, 12), our results did not show any significant difference in monopodal stability, which differ from most of the previous studies. McGuine et al. observed in 2000 that basketball players with poorer preseason unilateral balance values were seven times more prone to ankle sprains during the season9), and Soderman et al. reported similar findings for female soccer players, with the ones with lower scores for unilateral postural balance being more prone to leg-related injuries12). Similar results were found for unilateral stability of athletes by Watson et al., who assessed the monopodal postural sway by making soccer players maintain unilateral balance for 15 seconds, and those who were not able to perform it without touching down were classified as having abnormal postural sway. This group was the most affected by posterior ankle sprains19). Also, our findings contrast with the study of Trojian and McKeag in 2006, in which they found a positive association between monopodal support stability and ankle sprains11).
In addition, the results of stabilometric tests carried out in the volume period show that athletes with worse center-of-pressure values in the mediolateral plane while performing during right-leg monopodal support were more commonly injured during the two subsequent months, which comprised the pre-competition period. In spite of the fact that these results were found in monopodal stabilometry instead of bipodal stabilometry, these findings show the same trend ilustrated by the previous values of center-of-pressure spread found during the first part of the present study, in which injured athletes exhibited stability deterioration. Besides, these results support the research by McGuine et al. and Soderman et al., who reported in basketball players and soccer players, respectively, poorer unilateral stabilometric center-of-pressure values in subjects who were later found to be injured more frequently9, 12). These results are also in accord ance with those of Trojian and McKeag, who associated worse monopodal stabilometry with later ankle sprains in athletes11), and agree with those of Wang et al., who established in 2006 a correlation between poorer center-of-pressure mediolateral position and later ankle injuries10).
On the other hand, in 2001 and 1995, respectively, Beynnon et al. and Hopper et al. did not find data to support the value of postural balance as a predictor of ankle sprains14, 15), which differs from the rest of the studies and the present investigation. The same procedure was used by Willems et al. in 2005, who did not find significant differences in postural stability variables; however, these authors discovered that subjects with weaker control over their center of gravity were more prone to later suffering ankle sprains20).
Similar trends were seen for the results of both forms of stabilometric testing performed in the preseason period and the number of athletes injured in the volume period compared with the testing performed in the volume period and the number of athletes injured during the pre-competition period. Both sets of data point to athletes with higher values (and therefore poorer scores) for stabilometric variables being more prone to injuries in the subsequent periods. However, higher stabilometric variables were found for the bipodal stance in the first part, whereas higher stabilometric variables were found for the monopodal stance in the second part.
Based on the difference between the results of the parts of the present study, it is important to take into account that the injuries that occurred during the pre-competition period could have been influenced by other risk factors such as higher intensity of trainings or explosive actions, which are thought to be actions involving more damage21) and characteristic of this training period.
Also, it is important to indicate that the present investigation is the only study to date in which all lower extremity injuries were correlated with increases in postural sway. The rest of the investigation referred strictly to ankle-foot injuries.
In addition, certain limits of our study may have played a part in determining the lack of more significant differences. The low number of injuries recorded as a consequence of the small size of the sample might conceivably have contributed to this discrepancy in results. Indeed, the difference in number of athletes participating in both parts of the study could have affected the results due to the small size of the sample. Further research with a larger sample size is recommended, as well as inclusion of other age groups.
In conclusion, athletes who show higher center-of-pressure spread during bipodal stabilometry at the end of the preseason are more prone to injuries during the subsequent training period. Also, athletes who exhibit poorer stability in the mediolateral plane when performing right-leg monopodal support at the end of the volume period are more prone to injuries in the subsequent training period. As a practical application, inclusion of specific proprioceptive training in the training routines of athletes is recommended in order to improve stabilometric parameters and decrease and/or eliminate their role as risk factors.
REFERENCES
- 1.Freeman MA, Dean MR, Hanham IW: The etiology and prevention of functional instability of the foot. J Bone Joint Surg Br, 1965, 47: 678–685 [PubMed] [Google Scholar]
- 2.Paterno MV, Schmitt LC, Ford KR, et al. : Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med, 2010, 38: 1968–1978 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Riemann BL, Lephart SM: The sensorimotor system, part II: the role of proprioception in motor control and functional joint stability. J Athl Train, 2002, 37: 80–84 [PMC free article] [PubMed] [Google Scholar]
- 4.Lepers R, Bigard AX, Diard JP, et al. : Posture control after prolonged exercise. Eur J Appl Physiol Occup Physiol, 1997, 76: 55–61 [DOI] [PubMed] [Google Scholar]
- 5.Gribble PA, Hertel J, Denegar CR, et al. : The effects of fatigue and chronic ankle instability on dynamic postural control. J Athl Train, 2004, 39: 321–329 [PMC free article] [PubMed] [Google Scholar]
- 6.Nagy E, Toth K, Janositz G, et al. : Postural control in athletes participating in an ironman triathlon. Eur J Appl Physiol, 2004, 92: 407–413 [DOI] [PubMed] [Google Scholar]
- 7.Akbari M, Karimi H, Farahini H, et al. : Balance problems after unilateral lateral ankle sprains. J Rehabil Res Dev, 2006, 43: 819–824 [DOI] [PubMed] [Google Scholar]
- 8.Leanderson J, Eriksson E, Nilsson C, et al. : Proprioception in classical ballet dancers. A prospective study of the influence of an ankle sprain on proprioception in the ankle joint. Am J Sports Med, 1996, 24: 370–374 [DOI] [PubMed] [Google Scholar]
- 9.McGuine TA, Greene JJ, Best T, et al. : Balance as a predictor of ankle injuries in high school basketball players. Clin J Sport Med, 2000, 10: 239–244 [DOI] [PubMed] [Google Scholar]
- 10.Wang HK, Chen CH, Shiang TY, et al. : Risk-factor analysis of high school basketball-player ankle injuries: a prospective controlled cohort study evaluating postural sway, ankle strength, and flexibility. Arch Phys Med Rehabil, 2006, 87: 821–825 [DOI] [PubMed] [Google Scholar]
- 11.Trojian TH, McKeag DB: Single leg balance test to identify risk of ankle sprains. Br J Sports Med, 2006, 40: 610–613, discussion 613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Söderman K, Alfredson H, Pietilä T, et al. : Risk factors for leg injuries in female soccer players: a prospective investigation during one out-door season. Knee Surg Sports Traumatol Arthrosc, 2001, 9: 313–321 [DOI] [PubMed] [Google Scholar]
- 13.Murphy DF, Connolly DA, Beynnon BD: Risk factors for lower extremity injury: a review of the literature. Br J Sports Med, 2003, 37: 13–29 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hopper DM, Hopper JL, Elliott BC: Do selected kinanthropometric and performance variables predict injuries in female netball players? J Sports Sci, 1995, 13: 213–222 [DOI] [PubMed] [Google Scholar]
- 15.Beynnon BD, Renström PA, Alosa DM, et al. : Ankle ligament injury risk factors: a prospective study of college athletes. J Orthop Res, 2001, 19: 213–220 [DOI] [PubMed] [Google Scholar]
- 16.Asociación Médica Mundial: La Declaración de Helsinki en debate. Rev Med Uruguay, 2008, 24: 67–68 [Google Scholar]
- 17.Romero-Franco N, Martinez-Lopez E, Lomas-Vega R, et al. : Effects of proprioceptive training program on core stability and center of gravity control in sprinters. J Strength Cond Res, 2012, 26: 2071–2077 [DOI] [PubMed] [Google Scholar]
- 18.Kolt GS, Kirkby RJ: Epidemiology of injury in elite and subelite female gymnasts: a comparison of retrospective and prospective findings. Br J Sports Med, 1999, 33: 312–318 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Watson AW: Ankle sprains in players of the field-games Gaelic football and hurling. J Sports Med Phys Fitness, 1999, 39: 66–70 [PubMed] [Google Scholar]
- 20.Willems TM, Witvrouw E, Delbaere K, et al. : Intrinsic risk factors for inversion ankle sprains in male subjects: a prospective study. Am J Sports Med, 2005, 33: 415–423 [DOI] [PubMed] [Google Scholar]
- 21.Pastre CM, Carvalho Filho G, Monteiro HL, et al. : Lesões desportivas no atletismo: comparação entre informações obtidas em prontuários e inquéritos de morbidade referida. Rev Bras Med Esporte, 2004, 10: 1–8 [Google Scholar]