
Fig. 1. MRI findings evaluated for in each patient with IIH.
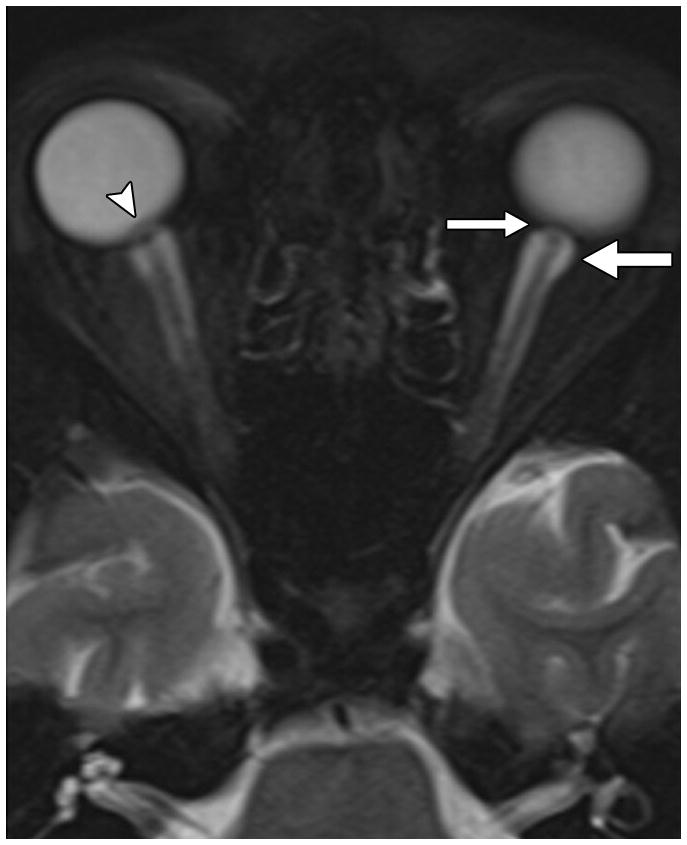
A. Orbital findings of ON head protrusion (arrowhead), posterior scleral flattening (thin arrow), and increased orbital peri-ON CSF (thick arrow) on a magnified axial T2-weighted fat-saturated image.
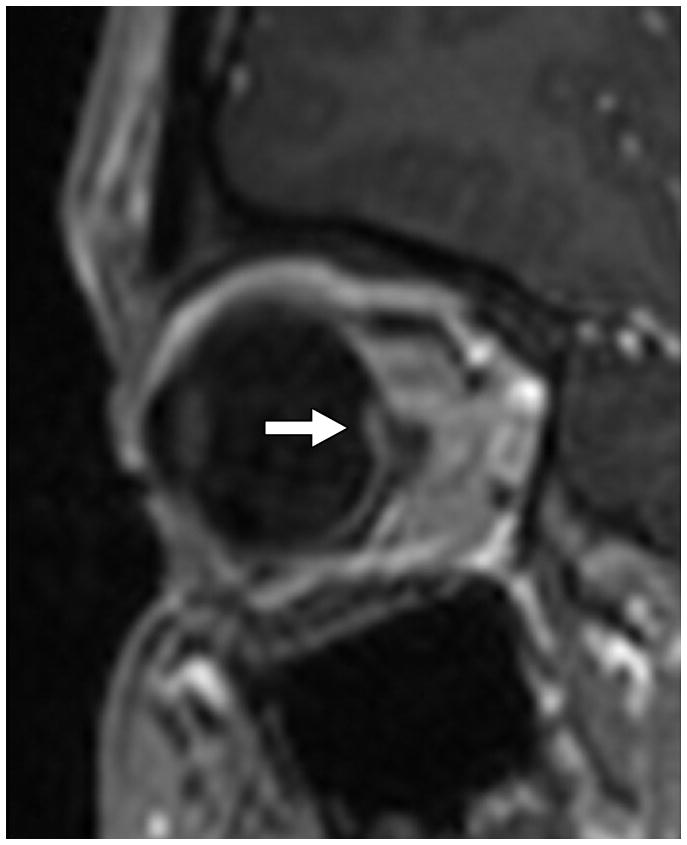
B. ON head enhancement and protrusion (arrow) on a magnified sagittal post-contrast volumetric T1-weighted image.
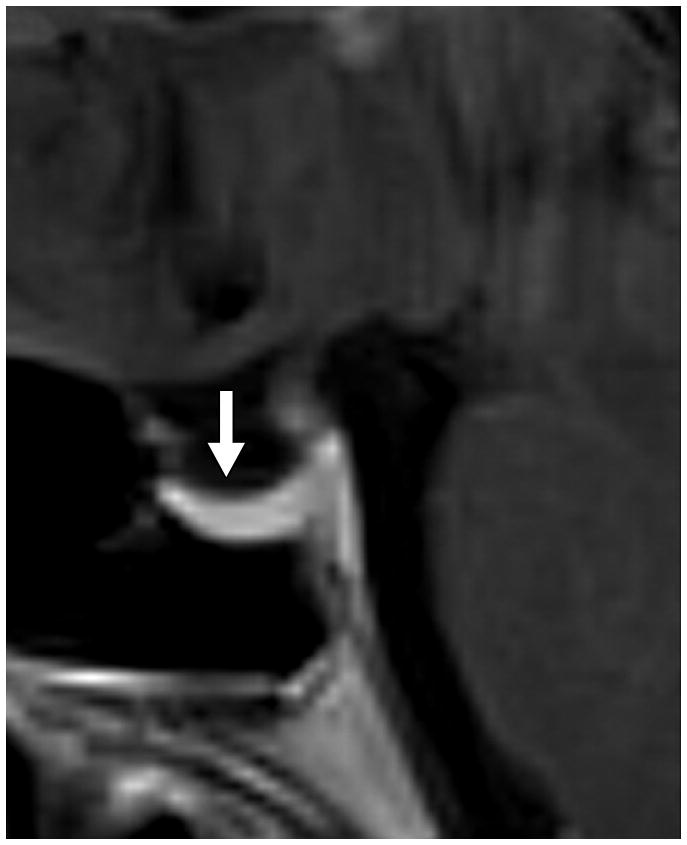
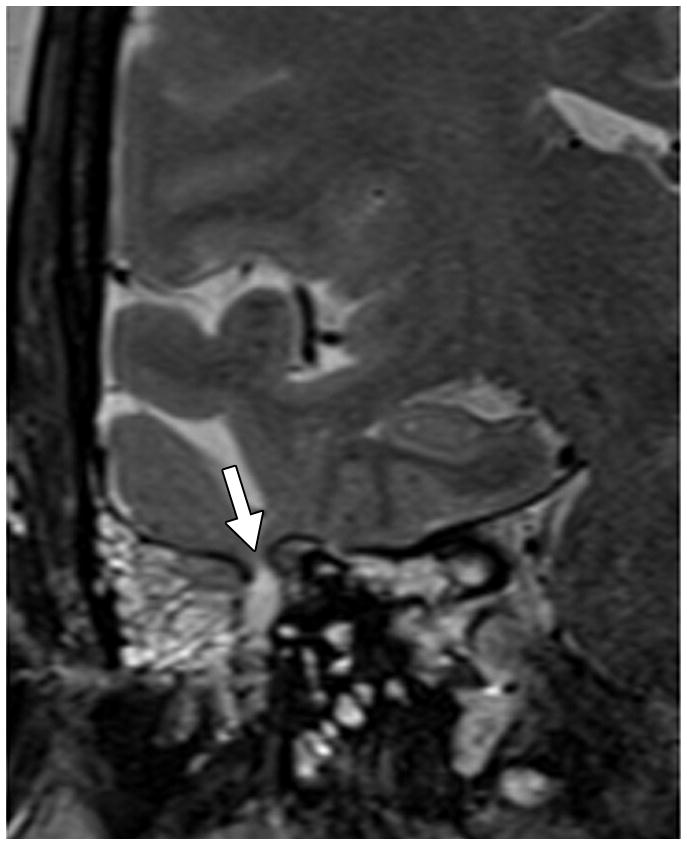
C. Pituitary grade. This was graded from I to V using the method of Yuh et al. The pituitary on this magnified mid-sagittal T1-weighted image depicted would be a category IV: superior concavity mild (>2/3) the height of the sella (arrow)
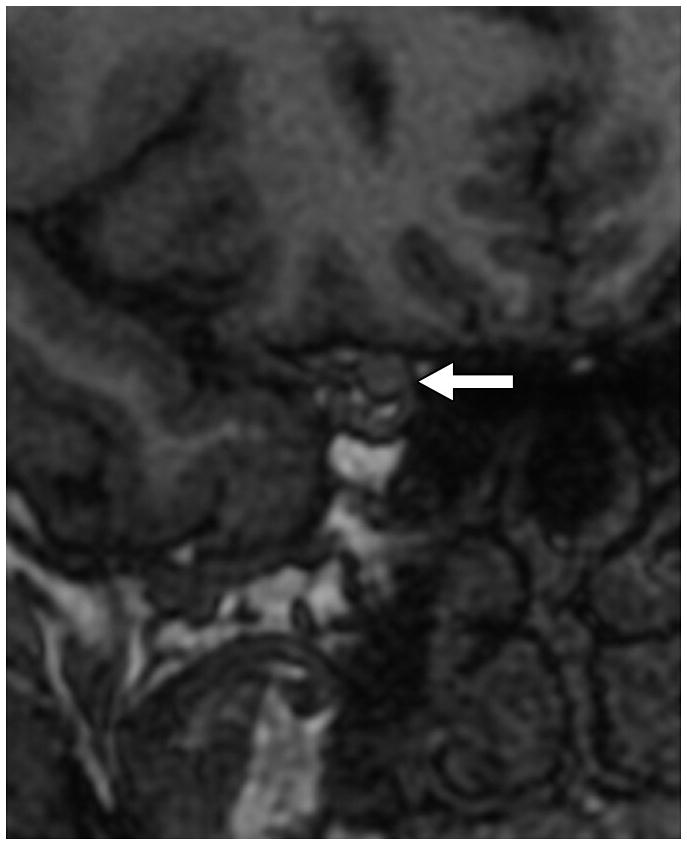
D. Optic canal width. Oblique coronal reformats of the volumetric Magnified reformatted volumetric T1-weighted dataset orthogonal to the axis of the intracanalicular ON were generated and the minimal diameter was measured. Arrow points to the ON.
E. Cephaloceles. These were defined as CSF or brain and CSF containing structures outside of the expected confines of the cranial vault. This coronal T2-weighted image shows multiple osteodural defects with CSF filling the right mastoid air cells.
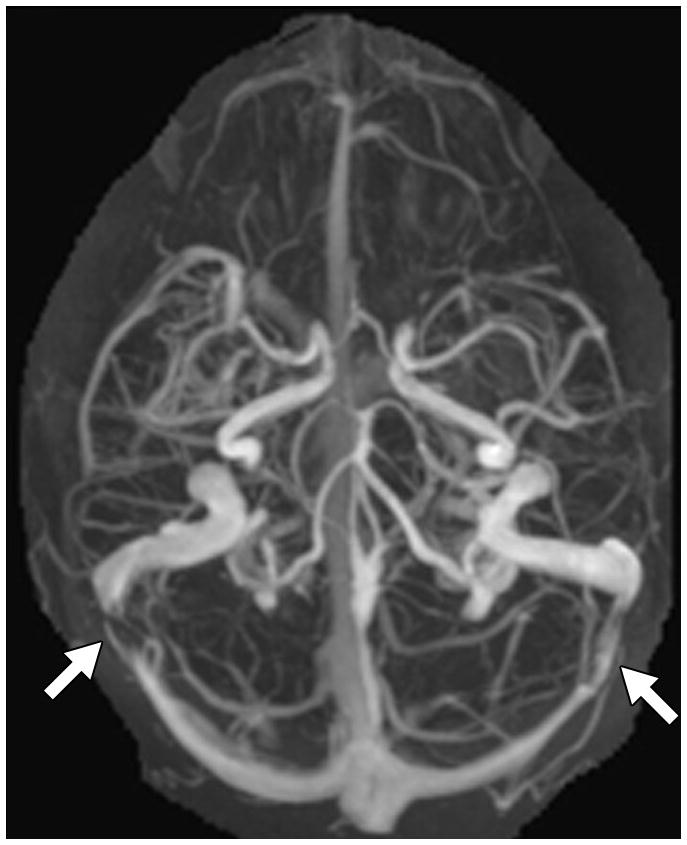
F. TSS on MRV. This was based on MIP images generated from either contrast-enhanced MRV (n=23) or 2D TOF MRVs (n=19). The image shows a cranio-caudal projection of a contrast-enhanced MRV with bilateral TSS (arrows).