
Figure 2.
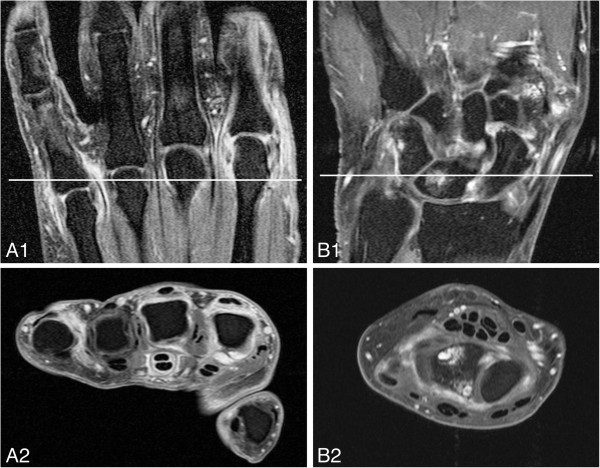
Subclinical inflammation visualised by magnetic resonance imaging of two different anticitrullinated peptide antibody–negative arthralgia patients without clinically detectable arthritis. Images show the metacarpophalangeal (MCP) joints and wrists of anticitrullinated peptide antibody (ACPA)–negative arthralgia patients without clinically detectable arthritis. The white lines in the top coronal images reflect the localisation of the bottom axial images. (A) Post–contrast enhancement coronal (A1) and axial (A2) T1-weighted fast spin echo (FSE) images with fat saturation showing enhancement of the MCP2, MCP3 and MCP5 joints, which is consistent with active synovitis. Also, pronounced tenosynovitis in the third flexor tendon is present, although tenosynovitis is not included in the OMERACT rheumatoid arthritis magnetic resonance imaging scoring system score and was not evaluated in the present study. This patient developed clinically detectable arthritis during follow-up. (B) Post–contrast enhancement coronal (B1) and axial (B2) T1-weighted FSE images with fat saturation showing bone marrow oedema (BME) and erosions (confirmed on the pre–contrast enhancement T1-weighted FSE sequence) in the lunate. Also, there is active synovitis in the intercarpal joint.