

Abstract
Background:
Until date, the importance of maternal health care services in reducing maternal mortality and morbidity has received a significant recognition. Most of the maternal deaths can be prevented if women have access to basic antenatal, natal and postnatal care. However, uptake of maternal health care services is far from universal even in settings where they are extensively available.
Aim:
The aim of this study is to assess the pattern and identify underlying factors on maternal health care utilization in rural areas of Bareilly.
Subjects and Methods:
This was a cross-sectional study was conducted during June-December 2011. Six villages were selected by convenience out of 99 villages in Bhojipura Block of Bareilly district, Uttar Pradesh to cover maximum number of women. All currently married women aged between 15 and 49 years who had delivered a child within last 1 year were interviewed by house-to-house survey and comprised the study unit. Their socioeconomic and demographic characteristics, reproductive history and knowledge of specific obstetric complications were taken. The information was gathered on various aspects of maternal-care utilization. In analyzing data, both bivariate and multivariate analyses were employed, using the Microsoft Excel and SPSS for Windows, Version 15.0 (SPSS Inc., Chicago, Illinois,USA).
Results:
Most (88.6%; 343/387) of pregnancies had registration for antenatal care (ANC). Majority (69.7%; 239/343) of them were registered between 16 and 24 weeks. Only 28.5% (110/343) of women received ANC from a private doctor. Maternal health care service utilization from health personnel was significantly associated with age at marriage ≥18 years, family size ≤3, birth order ≤2, nuclear family and higher socio-economic status. Most of the pregnancy related complications were found among women aged >30 years, with birth order ≥3, having birth interval <24 months, among Muslims, working mothers and among those belonging to joint family. Mother's education and husband's occupation were found to be strong predictors for the utilization of maternal health care using the logistic regression.
Conclusion:
Utilization of maternal health care services is high. However this can be improved by community based education program.
Keywords: Anemia, Antenatal care, Health care seeking behavior, Mother's education, Tetanus toxoid
Introduction
Utilization of health services is a complex behavioral phenomenon. Empirical studies of preventive and curative services have often found that the use of health services is related to the availability, quality and cost of services, as well as social structure, health beliefs and personal characteristics of the users.[1,2]
In developing countries, health seeking behaviors and health care services utilization patterns have been studied and the determinants have been classified in physical, socio-economic, cultural and political contexts.[3] Higher income and better social status are linked to better health. Larger the gap between the income and social strata, greater the differences exists in health status. Safe water and clean environment, healthy workplaces, better housing, communities and roads all contribute to good health. Greater support from families, friends, communities and good governance with political commitments is linked to better health also. Number of studies show that tendency in utilization of a health care services, government or private, formal or non-formal, usually vary, depending on factors such as age, gender, women's autonomy, living standard, economic status, severity of morbidity, availability of health infrastructure, type and cadre of health provider, etc.
Regarding utilization of maternal medical services, it is well-recognized that women's age plays an important role.[4,5] Mother's age may sometimes serve as a reflection for the women's build up knowledge of health care services, which may have a positive force on the use of health services. On the other hand, because of development in health care delivery system and improvement in educational opportunities for women in recent years, younger women might have an enhanced knowledge of available health care services and place more value upon modern medicine.
The child bearing functions of women, especially in developing countries, have been granted as a normal or routine process. Yet these valued and precious parts of life are among the most hazardous experiences that women often engage in without being aware of the risks or dangers that they are in. Maternal mortality ratio in India is 212/100,000 live births despite the existence of National program for improving the maternal and child health.[6] Most of the maternal deaths can be prevented if women have access to basic antenatal, natal and postnatal care. In India, these services are provided by government through a network of health centers at various levels in out-patient clinics, as well as through home visits by health workers.
Until date, the importance of maternal health care services in reducing maternal mortality and morbidity has received a significant recognition. Implementing and assuring utilization of effective maternity care for women in the developing world is not an easy task. In recent years, efforts to eliminate inequalities in the utilization of maternal health care services have been emphasized for the overall improvement of maternal health in developing countries. As a part of ongoing efforts to provide basic preventive and curative health services to all, government and non-governmental organizations have been expanding their health services in rural India. One of the purposes of this expansion was to make essential services available to all women and children.
In year 2005, Janani Suraksha Yojana’ was implemented countrywide to reduce overall maternal mortality ratio and infant mortality rate by promoting institutional deliveries from all the sections of society.[7] However, uptake of maternal health care services is far from universal even in settings where they are extensively available.
Understanding of the practices of the community regarding maternity care during pregnancy is required. Therefore, the present study was carried out to assess the pattern of utilization of health care services provided to women who delivered in last 1 year in Bhojipura Block of Bareilly district. The aim of this study is to assess the level and determinants of maternal health care utilization of married women aged 15-49 years who had delivered within last 1 year in Rohilkhand region.
Subjects and Methods
The cross-sectional study was conducted during June to December 2011. A sample size of 369 was calculated assuming a minimum of maternal health care service utilization of 64%.[6] To attain this sample size six villages were selected by convenience out of 99 villages in Bhojipura Block of Bareilly district, Uttar Pradesh to cover maximum number of women. All currently married women aged between 15 and 49 years who had delivered a child within last 1 year were interviewed using house to house survey. We examine the health seeking behavior of the mothers in terms of their antenatal care (ANC) services utilization. Institutional Ethical Clearance and informed consent from the mothers was taken and respondents were explained about the purpose of the study. A total of 387 women participated in the study.
A pretested questionnaire was used for interview. The interview consisted of both structured and open-ended questions. All currently married women aged 15-49 were involved in the study. The questionnaire asked mother's age at birth, birth order, residence, region, women's education and work status, socio-economic status using Modified Prasad Classification based on per capita monthly income, religion and household decision-making autonomy as predictor variables of maternal health care seeking behavior. Along with other items, their socio-economic and demographic characteristics, reproductive history and knowledge of specific obstetric complications were also taken. Women having more than one pregnancy related complication, only the most recent complication was considered to assess treatment-seeking behavior for pregnancy related complications. When both life-threatening and non-life-threatening complications were reported, the most recent life-threatening complication was considered as the reference complication. A woman with no life threatening complications, treatment-seeking behavior for the last non-life-threatening complication was assessed.
The information of maternal-care utilization, for each live birth in the last 1 year preceding the survey, a woman was asked if she had received ANC. If she did, she was asked how many months pregnant she was when she first received ANC, who administered the care, how many ANC visits she had in all, whether she had received tetanus toxoid injections during her pregnancy and if so, how many injections she had received, whether she had received iron/folic-acid tablets while she was pregnant, where she gave birth and who assisted with the delivery. At least 3 visits of mother to the provider with 2 tetanus toxoid injections and 100 tablets of iron and folic acid availed (100 mg of elemental iron and 500 μg of folic acid) was taken as operational definition for Minimum recommended ANC in the study.
There are five dichotomous dependent variables for maternal health care indicators: Whether or not mothers received at least two doses of tetanus toxoid vaccine; whether or not mothers received iron/folic-acid tablets; whether or not mothers received ANC from a health professional in an institutional setting, from a health worker at home, or from any other person; whether or not mothers received delivery care from a trained health professional; and whether or not the birth was delivered in a public or private medical institution. Trained health professionals include doctors, nurses, trained nurse/midwives and other formally trained personnel.
Several independent variables, both socio-economic and demographic, which could potentially influence the outcome, were included in the analysis. Mother's education was categorized into three groups: Illiterate, literate less than middle school complete and middle school complete and above. Mother's employment status was categorized into working and not working outside the home. Caste was divided into two groups: Those belonging to backward and under-represented communities (scheduled castes and scheduled tribes) and those belonging to upper castes. Religion was classified into Hindu, Muslim and others. Birth order was broken down into three categories: 1, 2-3 and 4+. Modified Prasad's classification was applied to measure the individual's socio-economic status.[8]
Along with considering various maternal care services separately, a composite index based on the utilization of various maternal care services is also constructed to better explain their utilization in the region. The different types of maternal care services considered for the construction of this composite index include: ANC, whether the mother received enough iron and folic acid tablets, whether the mother received two tetanus toxoid injections, whether the birth was delivered in a medical institution and whether the delivery was assisted by a trained health personnel. Responses to these questions are used to develop a composite index on the status of utilization of maternal care services. The utilization index is created using principal component analysis (PCA). The PCA approach applies a factor score to each woman who answered all the questions in the index. Essentially, the more positive, or 1, responses a woman provides, the higher her score. A higher score, therefore, indicates better access to care, maternal behaviors and experience. The scores is further used to rank the study participants into five categories namely, “Poor,” “Fair,” “Average,” “Good” and “Excellent.” This index is used as the dependent variable in the analysis. This is affected at a different level from individual factors so this variable reflects the nature of the utilization status at the community level.
Data entry and statistical analysis were performed using the Microsoft Excel and SPSS windows version 15.0 software. Both bivariate and multivariate analyses were employed. The odds ratios with 95% of the confidence intervals were calculated to assess the association between the independent variables and maternal health care utilization. Multinomial Logistic Regression analysis was performed using factors affecting Health Care Service Utilization for Pregnancy related complications.
Results
Out of the 387 women enrolled in the study, 88.6% (343/387) of pregnancies were registered for ANC. Only one quarter of the women were registered for ANC before 16 weeks of gestation. The majority (54.5%; 211/343) of the women received ANC by an auxiliary nurse midwife (ANM). About half (51.2%; 198/343) of the women received ANC at a sub center [Figures 1 and 2].
Figure 1.
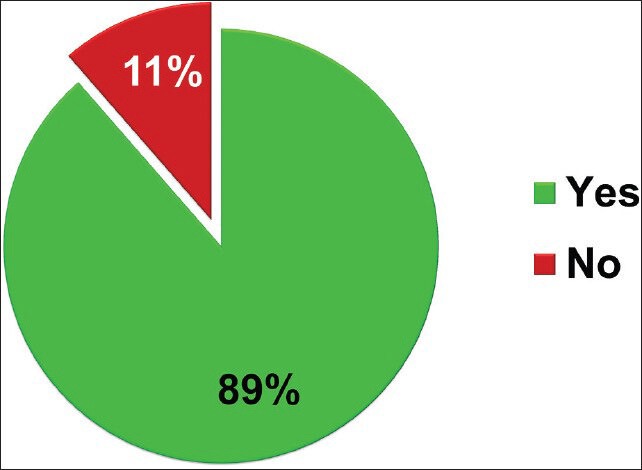
Distribution of women according to their registration status for antenatal care
Figure 2.
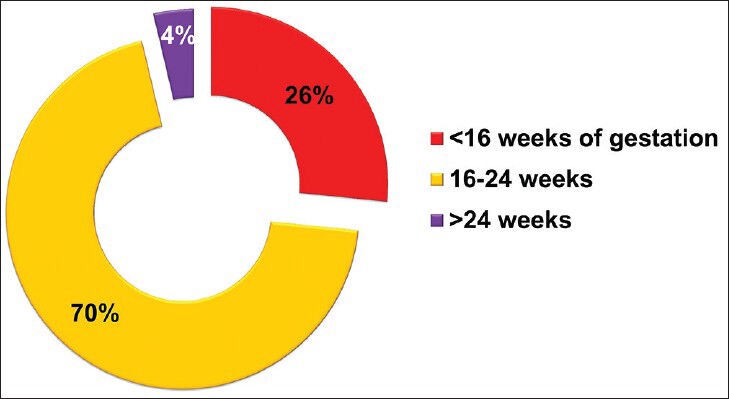
Distribution of women according to their gestational week of registration for antenatal care
Only 16.3% (56/343) of the pregnant females had minimum 3 ANC visits. Less than a quarter (23.6%; 13/56) of them was visited at their homes by a health worker for ANC checkups. Majority (83.7%; 287/343) of the respondents received two doses of tetanus toxoid while about one third (33.3%; 114/343) of them consumed at least 100 iron and folic acid tablets. About 50.4% (195/387) of the women had institutional deliveries while 32.5% (126/387) of the women were attended at home by a trained birth attendant at the time of delivery. Overall, 15.4% (60/387) of the respondents had a postpartum visit made by a health worker [Figure 3].
Figure 3.
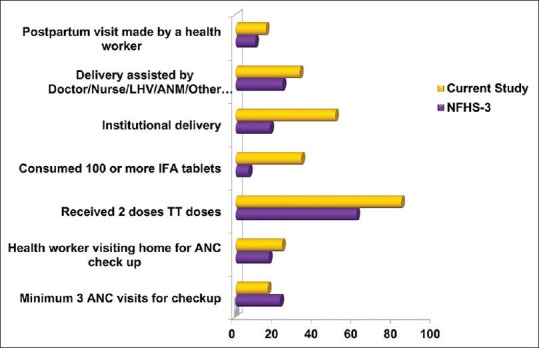
Comparison of utilization of antenatal, natal and postnatal care services in present study with National Family Health Survey-3
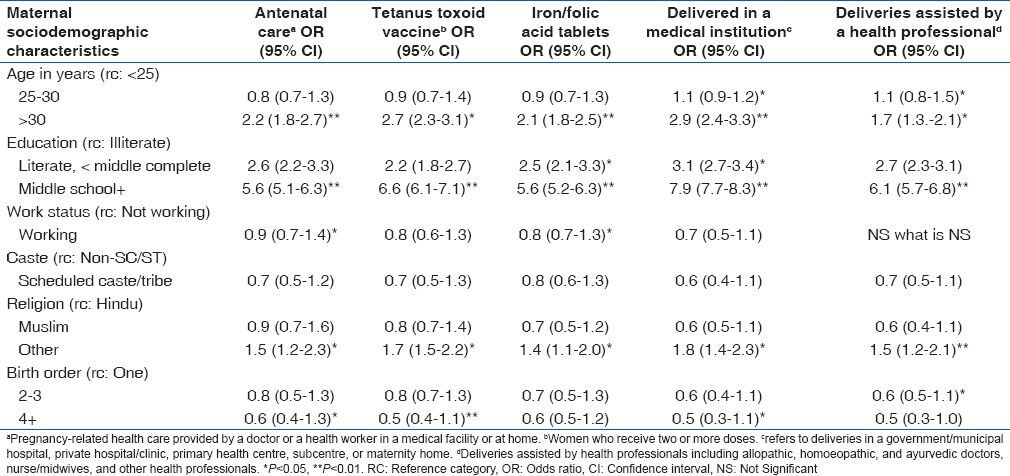
Young (<25 years) and older (>30 years) mothers are more likely to seek ANC than mothers in the age group 25-30 years. Education remains a consistently strong and significant predictor of maternal health-care utilization in all forms. In our study, education standard (Middle school +) of mother is proven to be a strong predictor of antenatal as well as natal care. With increase in educational status the utilization of maternal health care services seems to be increasing and this association is found to be statistically significant. Other important predictors affects maternal health care services positively are non-SC/ST caste, non-working status, belongs to religion other than Hindu and Muslim and primipara. Delivery in a medical institution is maternal health care service which affects maximally by all studied socio-demographic variables [Table 1].
Table 1.
ORs of maternal health care services utilization according to selected maternal sociodemographic characteristics
The index on utilization of maternal care services indicates Utilization of services by women aged 25-30 years is found to be very poor, while a greater percentage of women (25.9%; 55/213) with ≤2 order of births are found to be “excellent.” The use of maternal care declines sharply with increase in birth order.
The proportion of births where mothers utilized excellent maternal care services increases sharply with the increase in their education. As it is seen that only 10.8% (10/92) of illiterate mothers received “excellent” maternal care services compared with 49.6% (41/83) of mothers who completed at least high school.
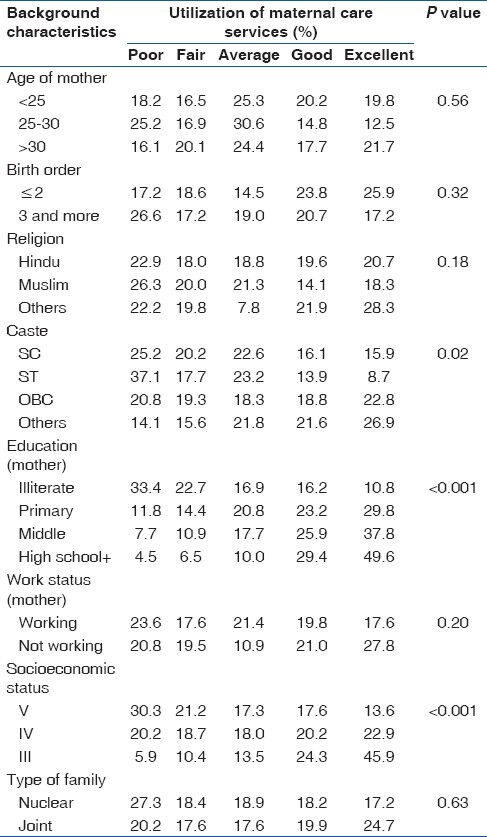
There is a substantial variation in the likelihood of utilization of maternal care services by religion. Only 18.3% (19/102) of the births to Muslim women received “excellent” maternal care services compared to 28.3% (8/28) of births to women belonging to religions other than Hindu and Islam. The utilization of maternal care services was “poor” among births to the scheduled tribe mothers compared with mothers of other caste/tribe. The likelihood of utilization of maternal care service was “excellent” among births to mothers of higher socio-economic status [Table 2].
Table 2.
Utilization of maternal care services by individual background characteristics
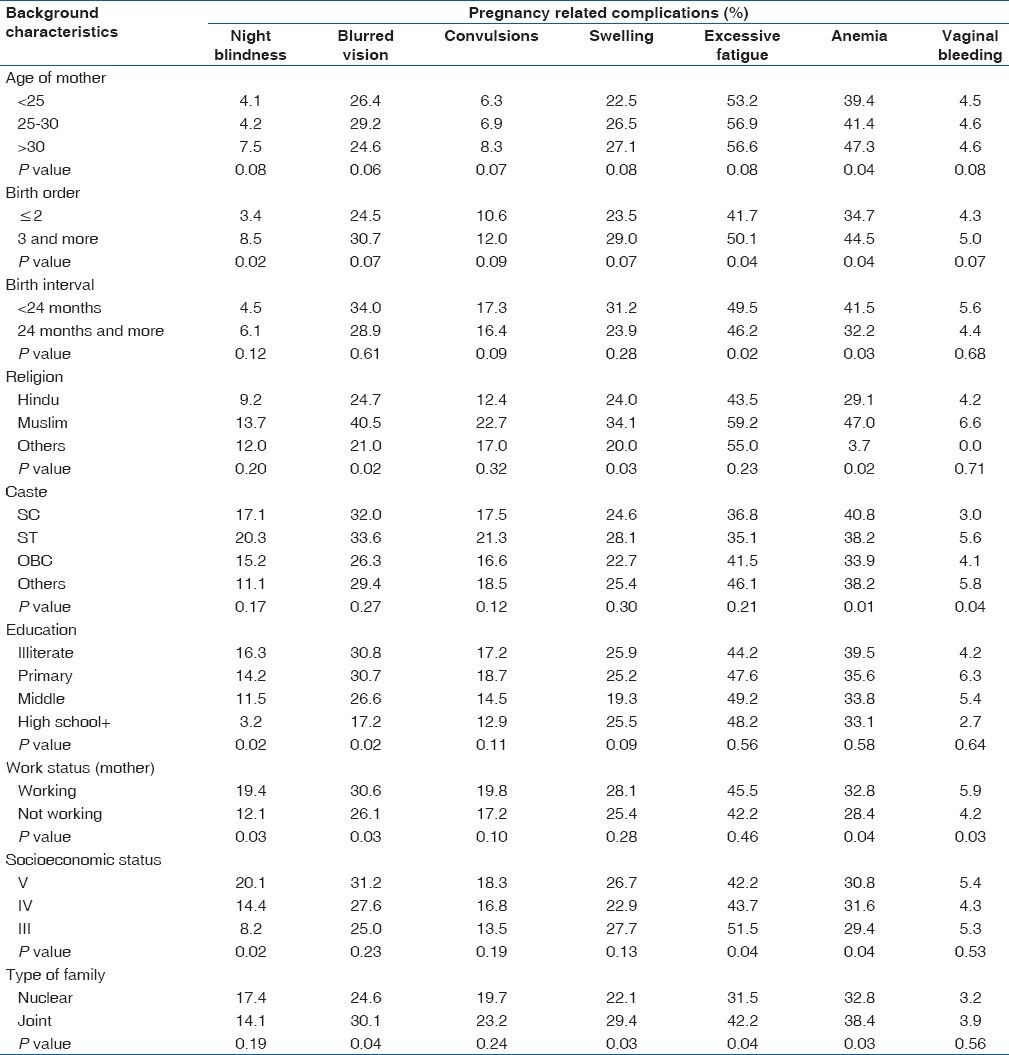
Most of the pregnancy complications were common in women who delivered baby with birth order ≥3, birth interval <24 months, Muslim by religion, working and belonged to joint family. Excessive fatigue is a major problem faced by women across all caste groups and it is followed by anemia. However, among the scheduled tribes blurred vision appears to be one of the main problems during the pregnancy. One interesting result, as the educated women are more likely to experience excessive fatigue compared to their illiterate counterparts was found. There is an overall decrease in the proportion of women suffering from various problems during pregnancy as the socio-economic status increases. In addition there is little variation in case of excessive fatigue and swelling, which tends to rise with an increase in the socioeconomic status. The reason for this is not clear. To summarize, it is observed that irrespective of socio-economic backgrounds, excessive fatigue and anemia continues to be two major problems during pregnancy among women. However in general, lower age of mother, lower birth order, longer birth interval coupled with higher education of women, higher socio-economic status act in favor of improving health of women during pregnancy [Table 3].
Table 3.
Distribution of pregnancy related complications according to sociodemographic characteristics of women
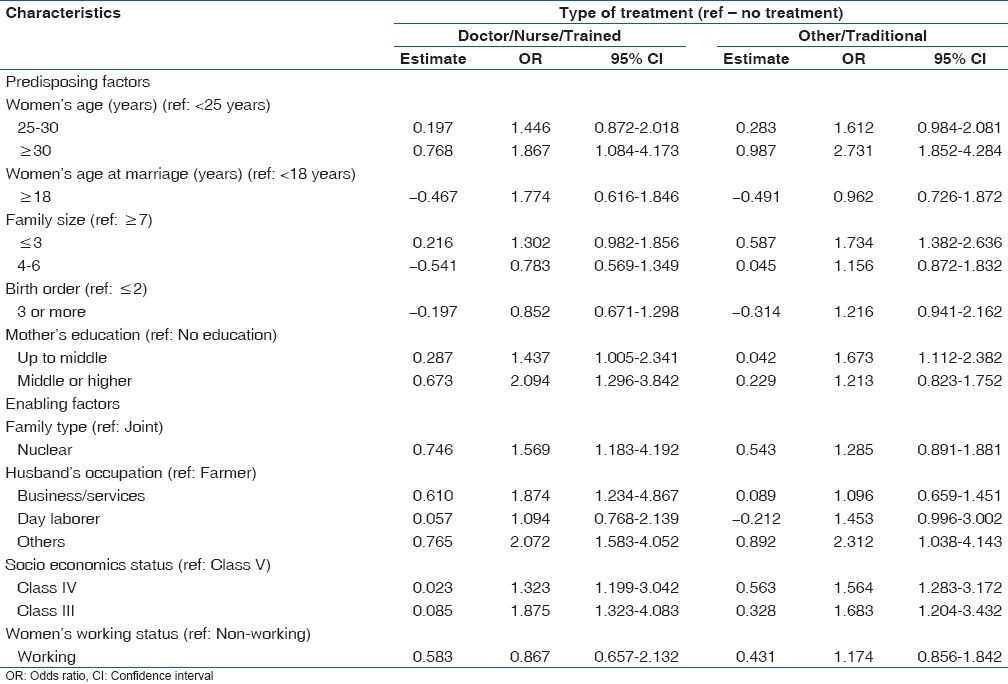
In the multinomial logistic regression model for health care use, older women had increased odds of using both modern and traditional health care service compared with younger women. Women who married at age <18 years were less likely to use both modern and traditional health care services compared with those who married at ≥18 years of age. Women with smaller family sizes and with higher previous pregnancy experiences were more likely to seek health care from qualified medical personnel. However, none of the above independent variables has a statistically significant impact upon health care utilization. Mother's education is likely to be associated with many of the other determinants considered in this study. The results indicate that female education has a net effect on maternal health service use, independent of other background characteristics, household socioeconomic status and access to health care services. Women with secondary or higher education are almost 1.9 times more likely to seek treatment from doctors/nurses to treat their antepartum morbidities. Among the enabling factors, husband's occupation seems to be an important determinant of maternal health care use, indicating that wives of men who work in business/service are more likely to seek treatment from a doctor or nurse compared with wives of farmers. Women from families in good economic condition are more likely to receive treatment from a doctor or nurse. However, the positive impact of higher economic status on health care use was not found to be statistically significant. The most important factor in explaining the utilization of maternal health care that arises from logistic regression is the mother's education and husband's occupation [Table 4].
Table 4.
Multinomial logistic regression analysis of factors affecting health care service utilization for pregnancy related complications
Discussion
Maternal health care service utilization from health personnel was significantly associated with age at marriage ≥18 years, family size ≤3, birth order ≤2, nuclear family and higher socio-economic status. Mother's education and husband's occupation were found to be predictors for the utilization of maternal health care using logistic regression. The main strength of the study is that the findings are based on current information collected directly from the beneficiaries not from any secondary data of any governmental/non-governmental agency and one potential limitation of this study could be only quantitative assessment of service utilization. The study doesn’t comment on the quality of services available and satisfaction/feedback of client towards services provided.
Behavioral model proposed that the use of health care services is a function of three sets of individual characteristics: (i) predisposing characteristics, e.g., age, household size, education, number of previous pregnancies, health-related attitude; (ii) enabling characteristics, i.e., income, characteristics of health care system and accesses and availability of health facilities; and (iii) need characteristics, i.e., characteristics of illness, perceived health status and expected benefit from treatments.[9]
ANC is one of the four most important pillars of safe motherhood along with family planning, safe delivery and essential obstetric care.[10] Majority of the women received ANC from a government functionary in our study. This is in contrast to the findings reported in Nigerian community where Private maternity center was the most preferred place for childbirth, while only 9.9% received ANC and 6.2% received two doses of tetanus toxoid. Private midwives and traditional birth attendants (TBAs) attended 49.4 and 42.0% of deliveries respectively.[11]
Utilization of all types of services is found to be better in our study area than National Family Health Survey findings except status of minimum 3 ANC visits to center. The reason behind this may be as essential services provided by ANM are available at their doorsteps during home visit so they think that there is no need to visit at centers. Better status of institutional deliveries in our study reflects clear cut effects of various maternal and child health program by Government of India especially Janani suraksha yojna to promote institutional delivery. Differences in findings are basically as national data is being diluted by low performance areas and our findings are confined to a particular area.
Utilization of health care services is affected by a multitude of factors. Several studies have attempted to identify and measure the effects of factors that contribute to differentiation in the utilization of health care services.[12] Review of literature across the globe suggests that these factors can be identified as cultural beliefs, socio-demographic status, women's autonomy, economic conditions, physical and financial accessibility and health services issue.[13]
A number of demographic and socio-economic factors such as education, religion and caste and birth order of baby have been identified as the major causes of poor utilization of primary health care services in our study also. Our findings are consistent to those reported by other studies.[14,15,16]
Parity, the number of children ever born, is found to be strongly associated with health seeking behavior. Studies show that primiparous women are consistently more likely to deliver with the assistance of a health professional than any other parity group. High parity women are the least likely to seek maternity care services due to greater confidence and cumulative experience.[17,18,19,20,21] On the other hand, nulliparous women seek early maternity care services.[22]
With regard to work status, one study made in four Indian states supports our findings that working mothers are less likely to deliver in a medical institution than non-working mothers.[12] Another local study, however, found that mothers’ work status does not significantly relate to utilization of maternal health care services.[15]
The odd of receiving ANC is lower for the 2nd-3rd births than first birth orders. The results of this study are consistent with those reported from different parts of the world.[23,24,25] Further explanations obtained from qualitative data indicated that women visit health institutions for ANC for their first birth than consecutive birth orders. Women who give birth to their first child without any complication do not want to visit health centers for ANC.
The importance of caste in life of an Indian (especially in case of Hindus) cannot be overlooked. Indian society is stratified into various societal layers on the basis of castes. There exist a social distance between the caste groups and the lower castes are not so much interested to avail the health care services due to some social constraints.[26] It was observed in our study that women of lower castes are less likely to avail for maternal care services compared to the higher caste women. This is mainly because membership to a particular caste has an impact on educational as well as economic status of women and also their attitude about health care provisions. When the influences of other intervening factors are controlled, education emerges as the single most important determinant of maternal health care utilization in India.[27] Education increases ANC awareness and brings about changes in health seeking behavior for better. It has also concluded by other studies that that as the caste status of women improves; there is an increase in the proportion of women receiving the package of ANC.[28]
The majority of previous studies on the utilization of maternal care services often considered various components independently.[19,29,30] Analysis conducted in this manner may perhaps not reflect the true pattern of utilization of services because some women may utilize only some but not all of the five components of the maternal care services. For example, one woman may go for ANC services but not deliver by Health Professional. By analyzing these aspects separately, one fails to judge the prevailing level of utilization of maternal care services.
In the present analysis we address the above-mentioned limitations using a theoretical framework developed by Andersen and Newman.[9] This approach incorporates both individual as well as program characteristics in addressing the utilization of maternal care services in rural areas of India. To capture the complexity of the various aspects of maternal care utilization we construct a composite index based on the various components of the maternal care services. The analysis based on such an index may provide a better picture of the utilization of maternal care services.
The Muslims have higher fertility rate.[6] It means higher birth orders and low birth intervals and these adversely affect health conditions during pregnancy. Apart from birth order it is also the interval between two births that exert a great influence on the woman's health. It is so because these women do not get proper time to recover from the strains of the previous pregnancy and hence fall easy victims to problems such as excessive fatigue and swelling in the following pregnancy.
Interesting results as the educated women are more likely to experience excessive fatigue and anemia compared with their illiterate counterparts. This is perhaps because of the fact that most of these women might be engaged in economic activities outside the house, which demands a considerable amount of their time and energy and prevent them from taking adequate rest. Statuses of pregnancy related complications is based on woman's self-reports and are not clinically tested. Hence, it limits the interpretation of finding to some extent.
Our study has shown a pattern of poor maternal health-seeking behavior for pregnancy related morbidity among women of less age, women with marriage age less than 18, large joint family size, working women with low education and low socio-economic status. Among those, there was a high preference for TBAs, who lack skills to respond to emergency obstetrical conditions. Various reasons given by our respondents with respect to their preference for delivering with TBAs, including greater accessibility, better interpersonal relationship, lower cost, greater convenience and freedom to use traditional birthing position have also been documented in other studies.[31,32]
The results from both bivariate and multivariate analysis confirmed the importance of mother's education on the utilization of health care services for pregnancy related complications. Woman's educational status retains a visible effect on maternal health service utilization, independent of other demographic characteristics, household's socioeconomic status and access to health care services. The strong influence of mother's education on the use of health care services is consistent with the findings from other studies.[1,5,17,25]
Conclusions
The study indicates that utilization of services was undoubtedly a reflection of their demographic and socio-economic characteristics. The study verifies widespread use of ANC, but it also reveals that antenatal visits occur mostly in 16-24 weeks of pregnancy. ANC utilization was associated with women's characteristics such as age, education, levels of education, working status, religion and birth order. Maternal health care service utilization from a doctor or nurse or a trained worker was significantly associated with age at marriage ≥ 18 years, family size ≤ 3, birth order ≤ 2, nuclear family and higher socio-economic status.
Utilization of maternity care services is of vital importance as it affects the well-being of the mother as well as her children. Thus government and other concerned agencies should also make efforts to develop better general community based education program so that women can have better understand gravity of maternity health care services and able to take proper measures recognizing that only healthy mother can give a healthy child and a healthy family.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Becker S, Peters DH, Gray RH, Gultiano C, Black RE. The determinants of use of maternal and child health services in Metro Cebu, the Philippines. Health Transit Rev. 1993;3:77–89. [PubMed] [Google Scholar]
- 2.Sarin AR. Underutilization of maternal health services. World Health Forum. 1997;18:67–8. [PubMed] [Google Scholar]
- 3.Kroeger A. Anthropological and socio-medical health care research in developing countries. Soc Sci Med. 1983;17:147–61. doi: 10.1016/0277-9536(83)90248-4. [DOI] [PubMed] [Google Scholar]
- 4.Elo IT. Utilization of maternal health-care services in Peru: The role of women's education. Health Transit Rev. 1992;2:49–69. [PubMed] [Google Scholar]
- 5.Fosu GB. Childhood morbidity and health services utilization: Cross-national comparisons of user-related factors from DHS data. Soc Sci Med. 1994;38:1209–20. doi: 10.1016/0277-9536(94)90186-4. [DOI] [PubMed] [Google Scholar]
- 6.Vol. 1. Deonar, Mumbai, India: International Institute for population Sciences (IIPS) and Macro International; 2007. International Institute for Population Sciences. National Family Health Survey (NFHS-3) [Google Scholar]
- 7.New Delhi: Ministry of Health and Welfare; 2005. Government of India. National Rural Health Mission (NRHM): Framework for Implementation. [Google Scholar]
- 8.Agarwal A. Social classification: The need to update in the present scenario. Indian J Community Med. 2008;33:50–1. doi: 10.4103/0970-0218.39245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Andersen R, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Mem Fund Q Health Soc. 1973;51:95–124. [PubMed] [Google Scholar]
- 10.Geneva: WHO; 1996. World Health Organization. Mother-Baby Package: Implementing Safe Motherhood in Countries: Practical Guide. [Google Scholar]
- 11.Osubor KM, Fatusi AO, Chiwuzie JC. Maternal health-seeking behavior and associated factors in a rural Nigerian community. Matern Child Health J. 2006;10:159–69. doi: 10.1007/s10995-005-0037-z. [DOI] [PubMed] [Google Scholar]
- 12.Sugathan K, Mishra V, Retherford R. Mumbai, India: International Institute for Population Sciences, and Honolulu: East-West Center, Population and Health Studies, USA; 2001. Promoting Institutional Deliveries in Rural India: The Role of Antenatal-Care Services. [Google Scholar]
- 13.Shaikh BT, Hatcher J. Health seeking behaviour and health service utilization in Pakistan: Challenging the policy makers. J Public Health (Oxf) 2005;27:49–54. doi: 10.1093/pubmed/fdh207. [DOI] [PubMed] [Google Scholar]
- 14.Leslie J, Gupta GR. Washington, D.C: International Centre for Research on Women; 1989. Utilization of Formal Services for Maternal Nutrition and Health Care. [Google Scholar]
- 15.Sharma SK, Vong-Ek P. Contextual influences on obstetric morbidity and related care seeking behaviour in Thailand. J Health Psychol. 2009;14:108–23. doi: 10.1177/1359105308097951. [DOI] [PubMed] [Google Scholar]
- 16.Pol G, Louis G, Thomas RK. New York: Plenum Press; 1992. The Demography of Health and Health Care. [Google Scholar]
- 17.Abbas AA, Walker GJ. Determinants of the utilization of maternal and child health services in Jordan. Int J Epidemiol. 1986;15:404–7. doi: 10.1093/ije/15.3.404. [DOI] [PubMed] [Google Scholar]
- 18.Mengistu M, James J. Determinants of antenatal care utilization in Arsi zone, Central Ethiopia. Ethiop J Health Dev. 1996;3:171–8. [Google Scholar]
- 19.Celik Y, Hotchkiss DR. The socio-economic determinants of maternal health care utilization in Turkey. Soc Sci Med. 2000;50:1797–806. doi: 10.1016/s0277-9536(99)00418-9. [DOI] [PubMed] [Google Scholar]
- 20.Bell J, Sian L, Curtis A, Siliva A. Calverton, Maryland, USA: ORC Macro; 2003. Trends in Delivery Care in Six Countries. DHS Analytical Studies NO. 7. [Google Scholar]
- 21.Kwast BE, Liff JM. Factors associated with maternal mortality in Addis Ababa, Ethiopia. Int J Epidemiol. 1988;17:115–21. doi: 10.1093/ije/17.1.115. [DOI] [PubMed] [Google Scholar]
- 22.Kaliszer M, Kidd M. Some factors affecting attendance at ante-natal clinics. Soc Sci Med D. 1981;15:421–4. doi: 10.1016/0160-8002(81)90061-7. [DOI] [PubMed] [Google Scholar]
- 23.Ferndez H. Voorburg: Netherlands International Statistical Institute; 1984. Analysis of information about mother – Child care taken from fertility surveys in Latin America. [Google Scholar]
- 24.Wong EL, Popkin BM, Guilkey DK, Akin JS. Accessibility, quality of care and prenatal care use in the Philippines. Soc Sci Med. 1987;24:927–44. doi: 10.1016/0277-9536(87)90286-3. [DOI] [PubMed] [Google Scholar]
- 25.Simkhada B, Teijlingen ER, Porter M, Simkhada P. Factors affecting the utilization of antenatal care in developing countries: Systematic review of the literature. J Adv Nurs. 2008;61:244–60. doi: 10.1111/j.1365-2648.2007.04532.x. [DOI] [PubMed] [Google Scholar]
- 26.Kopparty SN. Caste and utilization of health resources. East Anthropol. 1991;21:365–84. [Google Scholar]
- 27.Govindasamy P, Ramesh BM. Deonar, Mumbai, India: International Institute for population Sciences (IIPS) and Macro International; 1997. Maternal Education and Utilization of Maternal and Child Health Services in India. National Family Health Survey Subject Reports, No. 5. [Google Scholar]
- 28.Grover D, Singh R, Kaishtha KC, Gawari R, Singh S, Singh G. Visakhapatnam: Paper Presented at 24th Annual Conference of IASP; 2001. RCH-The Role of ANM. [Google Scholar]
- 29.Navaneetham K, Dharmalingam A. Utilization of maternal health care services in Southern India. Soc Sci Med. 2002;55:1849–69. doi: 10.1016/s0277-9536(01)00313-6. [DOI] [PubMed] [Google Scholar]
- 30.Matsumura M, Gubhaju B. Women's status, household structure and the utilization of maternal health services in Nepal. Asia Pac Popul J. 2001;16:23–44. [Google Scholar]
- 31.Fatusi AO, Ijadunola KT. Abuja, Nigeria: Federal Ministry of Health; 2003. National Study on Essential Obstetric Care Facilities in Nigeria. [Google Scholar]
- 32.Fatusi AO, Abioye-Kuteyi EA. Defining the Future Role of Traditional Birth Attendants in Reproductive Healthcare in Nigeria. Benin, Nigeria: Women Health and Action Research Center; 1998. Defining the traditional birth attendants: What we know about TBAs in Nigeria. [Google Scholar]