

Abstract
Objective
To estimate the relationship between the risk of preeclampsia and two thrombophilia gene single-nucleotide polymorphisms (SNPs), the factor V G1691A SNP and the prothrombin G20210A SNP.
Date Sources
A systematic search of the English-language literature up to November 2012 was performed using Medline and EMBASE. Search terms included “preeclampsia,” “thrombophilia,” “factor V Leiden,” “prothrombin gene 20210,” and their combinations.
Result(s)
Thirty-seven studies with 5048 preeclampsia patients and 6796 controls were included in the meta-analysis. We found that the prothrombin G20210A polymorphism was associated with an increased risk of all preeclampsia (pooled odds ratio (OR) = 1.81, 95% confidence interval (CI) 1.25–2.63) and severe preeclampsia (pooled OR = 3.02, 95%CI 2.06–4.45). Meanwhile, the pooled OR for the association between factor V Leiden and all preeclampsia was 1.60 (95%CI 1.28–2.00) and 2.45 (95%CI 1.63–3.69) for the cases of severe preeclampsia.
Conclusion(s)
This meta-analysis supports that the factor V G1691A SNP and the prothrombin G20210A SNP are associated with an increased risk for both preeclampsia overall and severe preeclampsia.
Introduction
Preeclampsia (PE), a complex disorder of pregnancy, is a major cause of maternal mortality worldwide, and is responsible for 15% to 20% of maternal mortality in developed countries [1]. It is thought to be a heterogeneous syndrome defined clinically by increased maternal blood pressure and proteinuria occurring after 20 weeks of gestation. The clinical manifestation of preeclampsia varies widely, from mild preeclampsia with only a moderate increase in blood pressure and proteinuria, to the most severe disorder with seizures and HELLP (hemolysis, elevated liver enzymes, and low platelets) syndrome, which greatly threatens the lives of pregnant women and their fetuses [2].
Despite many studies conducted previously, the etiology of PE remains unclear. Many hypotheses have been presented to explain the development of PE, including maternal and fatal genetic and environmental factors, classified into four categories: 1) immune maladaptation, 2) placental ischemia, 3) oxidative stress, and 4) genetic susceptibility [3]. Combinations of the many interactions between these categories may contribute to the etiology of preeclampsia. Among these, hypercoagulability, which plays a potential role in preeclampsia development, leads to decreased placental blood perfusion caused by microthrombi in placental blood vessels, eventually resulting in placental ischemia [4]. In the 1990s, factor V G1691A (also known as factor V Leiden, FVL) [5] and prothrombin G20210A (PT 20210) [6] were first reported to be related to a hypercoagulable state. Factor V 1691A allele and prothrombin 20210A allele were identified as risk factors for venous and arterial thrombosis. From then on these two genetic polymorphisms were inferred to be associated with PE and many studies have been conducted to explore the relationship between them. Several studies suggested that FVL [7]–[9] and PT 20210 polymorphism [9], [10] were associated with an increased risk of preeclampsia. However, other studies showed inconsistent results.
These inconsistent findings may be due to the differences in sample size, study design, ethnicity, and other aspects [11]. A meta-analysis is a useful tool with which to overcome these obstacles, owing to its increased statistical power. A previous attempt [12] has been made to explore the association between these two polymorphisms and the susceptibility of preeclampsia using a meta-analysis that included a relatively small number of studies. We therefore performed a meta-analysis to make a more precise assessment by adding more studies implemented in recent years. Furthermore, an evaluation of the relationship between these two SNPs and severe PE was conducted.
Materials and Methods
Search strategy
A computerized search of the English-language literature up to November 2012 was performed using Medline and EMBASE. We used the following search terms and the combinations thereof: “preeclampsia,” “thrombophilia,” “factor V Leiden,” and “prothrombin gene 20210.” The inclusion and exclusion criteria were as follows: (a) published studies with full text about the relationship between FVL or prothrombin G20210A and preeclampsia; (b) case-control studies; (c) studies with sufficient data to calculate odds ratio (OR) and 95% confidence interval (CI); (d) Reviews, letters, and single case reports were excluded; (e) if one group of patients was used in two or more studies, the study with the largest number of patients was selected.
Data extraction
Two investigators performed the literature search and screened the studies independently according to the inclusion and exclusion criteria. Agreements were reached after discussions if discrepancies occurred.
When all the eligible studies were included, we extracted the following information for each study: first author’s name, year of publication, study design, country, ethnicity (Caucasian, Asian or other ethnicities), and number of cases and controls for each FVL or prothrombin gene polymorphism genotype. In terms of disease definition, the criteria of the American College of Obstetricians and Gynecologists [13] and the National High Blood Pressure Education Program Working Group Report on High Blood Pressure in Pregnancy [14] were mostly used, in 13 [10], [15]–[26] and 6 [9], [27]–[31] studies, respectively, among which the definitions of preeclampsia and severe preeclampsia varied little. In these studies, preeclampsia was defined as systolic blood pressure ≥140 mmHg and diastolic blood pressure ≥90 mmHg, with the presence of proteinuria by 24-h urinary excretion exceeding 300 mg after 20 weeks of gestation. Severe preeclampsia was determined if one or more of the following features were present: blood pressure ≥160/110 mmHg; proteinuria >3+; oliguria; seizures; visual disturbances; headache; HELLP (hemolysis, elevated liver enzymes, and low platelets); right upper-quadrant pain; and thrombocytopenia. The remaining studies [7], [8], [32]–[52] used modified but relatively compatible diagnostic criteria.
In several studies, the authors classified the patients into two categories according to the severity of disease: severe PE group and not severe PE group while only severe preeclampsia patients were recruited into case group in some other studies. However, no similar classification was made in the remaining studies, in which each individual diagnosed as preeclampsia (not necessarily as severe preeclampsia) was included. To explore whether genetic thrombophilias increase the risk for preeclampsia in general or only for severe preeclampsia, we conducted two separate analyses: one involving all patients with preeclampsia (severe and not severe), and another separate analysis of severe preeclampsia in those studies that identified these cases separately.
Statistical analysis
Heterogeneity among studies was measured by the Q-statistic test and the I-squared statistical test. A fixed-effect model using the Mantel-Haenszel method was applied to calculate the pooled OR and 95% confident intervals (95%CI) if no or small heterogeneity was found. Otherwise a random-effect model using the DerSimonian-Laird method was used. Meta-regression was conducted to explore the source of heterogeneity, and influence analysis was performed when necessary. Studies with any zero cells were adjusted by adding 0.5 to each cell of the 2×2 table. Publication bias was assessed by funnel plot and Egger’s test. All analyses were performed using Stata 11.0 software (StataCorp LP, College Station, TX, USA).
Results
Based on our search criteria, a total of 42 studies were included in this analysis. Two studies [28], [36] were excluded because of the absence of FVL in either patient or control groups, one of which identified this SNP in a Japanese population[28]. With regard to ethnic background, it was difficult to identify the ethnic origin of individuals in three studies [24], [31], [34], which were therefore excluded. Ultimately 37 studies were included in our meta-analysis, with 23 studies evaluating the PT 20210 polymorphism and 35 analyzing the FVL. The study selection process is presented in Figure 1. In terms of study design, eight studies [21], [26], [37]–[42] were prospectively designed and the rest were retrospective case-control studies. The data of each group are shown in the tables. In these studies, homozygotes of factor V 1691A allele and prothrombin 20210A allele were rarely detected in either the patient or the control groups, so the heterozygotes and homozygotes of each thrombophilia gene mutation were considered together. Table 1 and 2 present the results of studies that include cases of preeclampsia (not necessarily defined as severe), and Table 3 and 4 show the studies that include cases identified as severe preeclampsia. In twelve studies [15]–[17], [22], [25], [37]–[40], [48], [49], [52], only severe preeclampsia was defined and in seven[9], [10], [18], [32]–[35], the authors defined both preeclampsia and severe preeclampsia and performed further analysis of the association between the two polymorphisms and severe preeclampsia after analysis for all preeclampsia. In the remaining studies, the authors only defined preeclampsia and didn’t describe the distribution of mild and severe cases. However, in Mello’s study [10], which included 402 mild PE cases and 406 severe PE cases, the investigators analyzed mild PE and severe PE separately because of the high percentage of patients with severe preeclampsia, which did not reflect the prevalence of the disease in the general population.
Figure 1. Flow diagram of meta-analysis literature search results.
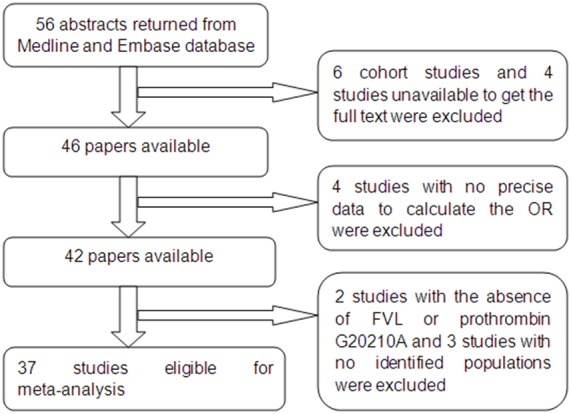
Table 1. Case-control studies of Prothrombin 20120 G-A Polymorphism and All Preeclampsia.
| study | country | ethnicity | cases | controls | OR | 95%CI | ||
| GG | GA/AA | GG | GA/AA | |||||
| De Groot(1999) | Netherland | Caucasian | 158 | 5 | 157 | 6 | 0.83 | (0.25–2.77) |
| Kupferminc(2000) | Israel | Caucasian | 73 | 7 | 151 | 5 | 2.90 | (0.90–9.44) |
| Higgins(2000) | Australia | Caucasian | 134 | 5 | 116 | 3 | 1.44 | (0.34–6.17) |
| D’Elia(2002) | Italy | Caucasian | 57 | 1 | 73 | 1 | 1.28 | (0.08–20.92) |
| Morrison(2002) | Scotland | Caucasian | 396 | 4 | 164 | 0 | 3.73 | (0.20–69.74) |
| Prochazk(2003) | Czech | Caucasian | 37 | 1 | 50 | 0 | 4.04 | (0.16–102.0) |
| Fabbro(2003) | Italy | Caucasian | 50 | 2 | 78 | 2 | 1.56 | (0.21–11.43) |
| Driul(2005) | Italy | Caucasian | 38 | 1 | 63 | 1 | 1.66 | (0.10–27.29) |
| Mello(2005) | Italy | Caucasian | 386 | 16 | 397 | 5 | 3.29 | (1.19–9.07) |
| Demir(2006) | Turkey | Caucasian | 65 | 5 | 95 | 7 | 1.04 | (0.32–3.43) |
| Yalinkaya(2006) | Turkey | Caucasian | 96 | 4 | 98 | 2 | 2.04 | (0.36–11.41) |
| Hiltunen(2009) | Finland | Caucasian | 244 | 4 | 673 | 6 | 1.84 | (0.52–6.57) |
| Best(2009) | US | American Indian | 86 | 1 | 164 | 1 | 1.91 | (0.12–30.86) |
| Kahn(2009) | Canada | Caucasian | 110 | 3 | 435 | 8 | 1.48 | (0.39–5.68) |
| Seremak-Mrozikiewicz(2010) | Poland | Caucasian | 104 | 5 | 395 | 5 | 3.80 | (1.08–13.37) |
| Malek-Khosravi(2012) | Western Iran | Caucasian | 194 | 4 | 98 | 3 | 0.67 | (0.15–3.07) |
| Pooled(M-H) | 1.81 | (1.25–2.63) | ||||||
Q = 8.10, p = 0.920, I2 = 0.0%.
Table 2. Case-control studies of Factor V Leiden Polymorphism and All Preeclampsia.
| study | country | ethnicity | cases | controls | OR | 95%CI | ||
| GG | GA/AA | GG | GA/AA | |||||
| Lindoff(1997) | Sweden | Caucasian | 39 | 11 | 45 | 5 | 2.54 | (0.81–7.93) |
| Mimuro(1998)a | Australia | 83% Caucasian | 46 | 4 | 149 | 1 | 12.96 | (1.41–118.83) |
| De Groot(1999) | Netherland | Caucasian | 147 | 16 | 148 | 15 | 1.07 | (0.51–2.25) |
| Mello(1999) | Italy | Caucasian | 34 | 12 | 77 | 3 | 9.06 | (2.40–34.18) |
| O’Shaughnessy(1999) | UK | Caucasian | 268 | 15 | 94 | 6 | 0.88 | (0.33–2.33) |
| Kim(2001) | US | Caucasian | 235 | 15 | 241 | 12 | 1.28 | (0.59–2.80) |
| D’Elia(2002) | Italy | Caucasian | 55 | 3 | 71 | 3 | 1.29 | (0.25–6.64) |
| Morrison(2002) | Scotland | Caucasian | 377 | 17 | 155 | 8 | 0.87 | (0.37–2.07) |
| Prochazka(2003) | Czech | Caucasian | 34 | 4 | 47 | 3 | 1.84 | (0.39–8.78) |
| Fabbro(2003) | Italy | Caucasian | 49 | 3 | 76 | 4 | 1.16 | (0.25–5.42) |
| Prasmusinto(2004) | Germany/Croatia | Caucasian | 36 | 4 | 71 | 1 | 7.79 | (0.85–73.20) |
| Faisel(2004) | Finland | Caucasian | 126 | 7 | 108 | 4 | 1.50 | (0.43–5.26) |
| Driul(2005) | Italy | American Indian | 35 | 4 | 62 | 2 | 3.54 | (0.62–20.33) |
| Davalos(2005) | Mexican | Caucasian | 31 | 2 | 60 | 2 | 1.94 | (0.26–14.41) |
| Mello(2005) | Italy | Caucasian | 389 | 13 | 389 | 13 | 1.00 | (0.46–2.18) |
| Demir(2006) | Turkey | Caucasian | 60 | 10 | 97 | 5 | 3.23 | (1.05–9.92) |
| Yalinkaya(2006) | Turkey | Caucasian | 94 | 6 | 96 | 4 | 1.53 | (0.42–5.60) |
| Hiltunen(2009) | Finland | Caucasian | 238 | 10 | 663 | 16 | 1.74 | (0.78–3.89) |
| Best(2009) | US | American Indian | 82 | 5 | 159 | 6 | 1.62 | (0.48–5.60) |
| Kahn(2009) | Canada | Caucasian | 107 | 6 | 421 | 22 | 1.07 | (0.42–2.71) |
| Seremak-Mrozikiewicz(2010) | Poland | Caucasian | 99 | 10 | 386 | 14 | 2.78 | (1.20–6.46) |
| Dissanayaka(2012) | Sri Lanka | Caucasian | 168 | 7 | 169 | 2 | 3.52 | (0.72–17.20) |
| Malek-Khosravi(2012) | Western Iran | Caucasian | 183 | 15 | 93 | 8 | 0.95 | (0.39–2.33) |
| Pooled(M-H) | 1.60 | (1.28–2.00) | ||||||
Q = 26.02, p = 0.251, I2 = 15.5%.
a: 83% of the cases were Caucasian and 17% were Asian.
Table 3. Case-control studies of Prothrombin 20120 G-A Polymorphism and Severe Preeclampsia.
| study | country | ethnicity | cases | controls | OR | 95%CI | ||
| GG | GA/AA | GG | GA/AA | |||||
| Kupferminc(1999) | Israel | Caucasian | 32 | 2 | 107 | 3 | 2.23 | (0.36–13.93) |
| Kupferminc(2000) | Israel | Caucasian | 58 | 5 | 122 | 4 | 2.63 | (0.68–10.16) |
| Kupferminc(2000) | Israel | Caucasian | 50 | 5 | 151 | 5 | 3.02 | (0.84–10.86) |
| Livingston(2001)a | US | 60% African American | 110 | 0 | 96 | 1 | 0.29 | (0.01–7.23) |
| Alfirevic(2001)b | UK | 90% Caucasian | 61 | 2 | 42 | 2 | 0.69 | (0.09–5.08) |
| Tempfer(2004) | Austria | Caucasian | 23 | 1 | 23 | 1 | 1.00 | (0.06–16.97) |
| Koleva(2005) | Bulgaria | Caucasian | 36 | 3 | 99 | 4 | 2.06 | (0.44–9.67) |
| Gerhardt(2005) | German | Caucasian | 93 | 4 | 271 | 6 | 1.94 | (0.54–7.04) |
| Mello(2005) | Italy | Caucasian | 362 | 44 | 398 | 8 | 6.05 | (2.81–13.02) |
| Demir(2006) | Turkey | Caucasian | 29 | 5 | 95 | 7 | 2.34 | (0.69–7.93) |
| Seremak-Mrozikiewicz 2010) | Poland | Caucasian | 63 | 5 | 395 | 5 | 6.27 | (1.76–22.28) |
| Malek-Khosravi(2012) | Western Iran | Caucasian | 68 | 2 | 98 | 3 | 0.96 | (0.16–5.90) |
| Pooled(M-H) | 3.02 | (2.06–4.45) | ||||||
Q = 11.65, p = 0.39, I2 = 5.8%.
a: 60% of the cases were African American, 40% were white Caucasian;
b: 90% of the cases were Caucasian and 10% were non-Caucasian.
Table 4. Case-control studies of Factor V Leiden Polymorphism and Severe Preeclampsia.
| study | country | ethnicity | cases | controls | OR | 95%CI | ||
| GG | GA/AA | GG | GA/AA | |||||
| Dizon-Townson(1996)a | US | 94% Caucasian | 144 | 14 | 386 | 17 | 2.21 | (1.06–4.59) |
| Kupferminc(1999) | Israel | Caucasian | 25 | 9 | 103 | 7 | 5.30 | (1.80–15.60) |
| van Pampus(1999) | Netherland | Caucasian | 267 | 16 | 66 | 1 | 4.20 | (0.55–32.15) |
| Rigo(2000) | US | Caucasian | 98 | 22 | 98 | 3 | 7.33 | (2.13–25.30) |
| Tempelhoff(2000) | Germany | Caucasian | 23 | 6 | 58 | 3 | 5.04 | (1.16–21.88) |
| Kupferminc(2000) | Israel | Caucasian | 48 | 15 | 118 | 8 | 4.61 | (1.83–11.58) |
| Livingston(2001)b | US | 60% AfricanAmerican | 105 | 5 | 94 | 3 | 1.49 | (0.35–6.41) |
| Alfirevic(2001)c | UK | 90% Caucasian | 62 | 1 | 41 | 3 | 0.22 | (0.02–2.19) |
| Kim(2001) | US | Caucasian | 158 | 11 | 241 | 12 | 1.40 | (0.60–3.25) |
| Currie(2002) | Australia | Caucasian | 42 | 4 | 40 | 6 | 0.64 | (0.17–2.42) |
| Tempfer(2004) | Austria | Caucasian | 21 | 3 | 22 | 2 | 1.57 | (0.24–10.36) |
| Koleva(2005) | Bulgaria | Caucasian | 29 | 10 | 97 | 6 | 5.58 | (1.87–16.64) |
| Gerhardt(2005) | German | Caucasian | 90 | 7 | 255 | 22 | 0.90 | (0.37–2.18) |
| Mello(2005) | Italy | Caucasian | 338 | 68 | 391 | 15 | 5.24 | (2.94–9.34) |
| Demir(2006) | Turkey | Caucasian | 28 | 6 | 97 | 5 | 4.16 | (1.18–14.64) |
| Seremak-Mrozikiewicz(2010) | Poland | Caucasian | 62 | 6 | 386 | 14 | 2.67 | (0.99–7.20) |
| Malek-Khosravi(2012) | Western Iran | Caucasian | 66 | 4 | 93 | 8 | 0.70 | (0.20–2.44) |
| Pooled(D-L) | 2.45 | (1.63–3.69) | ||||||
Q = 36.45, p = 0.003, I2 = 56.1%.
a: 94% of the cases were white Caucasian, 3% Hispanic, 2% Asian, 0.8% African and 0.4% Native American.
b: 60% of the cases were African American, 40% were white Caucasian;
c: 90% of the cases were Caucasian and 10% were non-Caucasian.
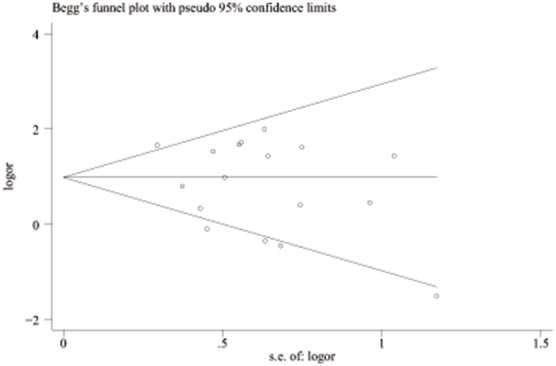
Table 1 lists the 16 studies (2296 cases and 3262 controls) that evaluated the association between PT 20210 polymorphism and all preeclampsia [9], [10], [18]–[21], [26], [27], [33], [35], [42]–[47]. The pooled OR was 1.81 (95%CI 1.25–2.63) with a Q statistic for heterogeneity of 8.10 (p = 0.920). No heterogeneity was found (I 2 = 0.0%), and the fixed model was used. These results are shown graphically in Figure 2. Figure 3 is the funnel plot showing the distribution of the individual measures of these studies. No publication bias was suggested by the funnel plot.
Figure 2. Forest plot of OR with 95%CI of all preeclampsia associated with the prothrombin G20210A polymorphism by fixed model.

Black square means value of OR, and the size of the square means inversely proportional to its variance. Horizontal line means 95% confience interval (CI) of OR. Black diamond means pooled results.
Figure 3. Begg’s funnel plot of publication bias test of all preeclampsia associated with the prothrombin G20210A polymorphism. LogOR means nature logarithm of OR (odds ratio).
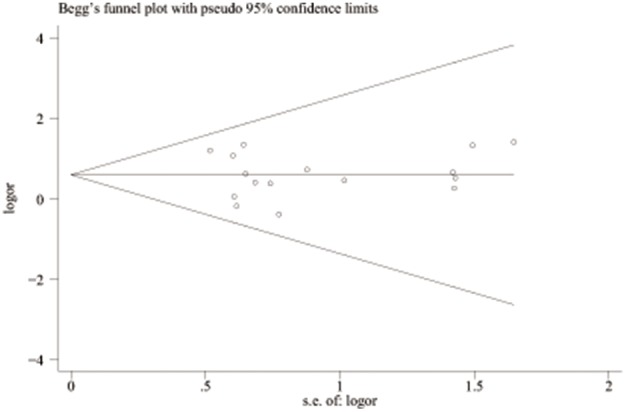
Horizontal line means the summary estimate, while the sloping lines mean the expected 95% confidence interval.
The effect of the PT 20210 polymorphism and severe preeclampsia is shown in Table 3. There are 12 studies involving a total of 1063 cases and 1946 controls[9], [10], [16]–[18], [22], [25], [33], [35], [38], [48], [49]. Only two studies [9], [10] reported a significant association between this polymorphism and severe preeclampsia. The pooled OR was 3.02 (95%CI 2.06–4.45) with p heterogeneity of 0.390. The results are shown in Figure 4. The funnel plot suggests a potential publication bias (Figure 5). Influence analyses, in which pooled OR are calculated omitting one study at a time, demonstrated that the results were influenced by Mello’s study [10] to some extent. The pooled OR decreased significantly from 3.02 (95%CI 2.06–4.45) to 2.08 (95%CI 1.31–3.32) after the omission of this study.
Figure 4. Forest plots of OR with 95%CI of severe preeclampsia associated with the prothrombin G20210A polymorphism in fixed model.

Black square means value of OR, and the size of the square means inversely proportional to its variance. Horizontal line means 95% confience interval (CI) of OR. Black diamond means pooled results.
Figure 5. Begg’s funnel plot of publication bias test of severe preeclampsia associated with the prothrombin G20210A polymorphism.
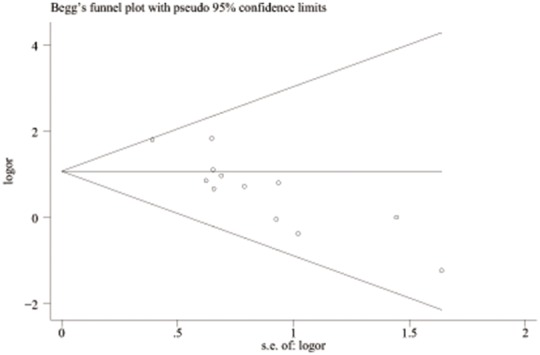
LogOR means nature logarithm of OR (odds ratio). Horizontal line means the summary estimate, while the sloping lines mean the expected 95% confidence interval.
Table 2 summarizes the analysis of 23 studies involving 3131 patients and 4036 controls that assessed the association between FVL and all preeclampsia [7]–[10], [19]–[21], [23], [26], [27], [29], [30], [32], [33], [35], [41], [42], [44]–[47], [50], [51]. Meta-analysis revealed a significant association between FVL and preeclampsia (pooled OR = 1.60, 95% CI 1.28–2.00, p = 0.251, I 2 = 15.5%) when a fixed model was applied (Figure 6). The funnel plot shows obvious evidence of publication bias in the lack of small negative studies (Figure 7).
Figure 6. Forest plots of OR with 95%CI of all preeclampsia associated with FVL in fixed model.

Black square means value of OR, and the size of the square means inversely proportional to its variance. Horizontal line means 95% confience interval (CI) of OR. Black diamond means pooled result.
Figure 7. Begg’s funnel plot of publication bias test of all preeclampsia associated with FVL.
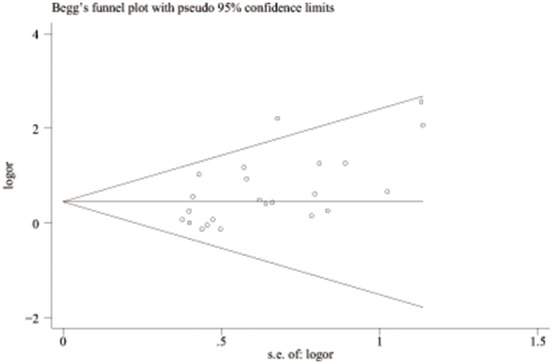
LogOR means nature logarithm of OR (odds ratio). Horizontal line means the summary estimate, while the sloping lines mean the expected 95% confidence interval.
Seventeen studies with 1814 patients and 2721 controls evaluated the association between FVL and severe preeclampsia, as shown in Table 4 [9], [10], [15]–[17], [22], [25], [32], [33], [35], [37]–[40], [48], [49], [52]. Obvious evidence of heterogeneity (Q = 36.45, p = 0.003, I 2 = 56.1%) was found between studies. Thus, a random model was used for which the pooled OR was 2.45 (95% CI 1.63–3.69). The results are shown graphically in Figure 8. Figure 9 is the funnel-plot analysis, which seems to be asymmetric. However, Egger’s test suggests no obvious evidence of publication bias (Egger’s test p = 0.246).
Figure 8. Forest plots of OR with 95%CI of severe preeclampsia associated with FVL in random model.

Black square means value of OR, and the size of the square means inversely proportional to its variance. Horizontal line means 95% confience interval (CI) of OR. Black diamond means pooled results.
Figure 9. Begg’s funnel plot of publication bias test of severe preeclampsia associated with FVL.
LogOR means nature logarithm of OR (odds ratio). Horizontal line means the summary estimate, while the sloping lines mean the expected 95% confidence interval.
Discussion
Preeclampsia is multifactorial gestational vascular complication that greatly threatens the life of pregnant women and their fetuses. The etiology of preeclampsia remains complex. Early studies reported that thrombophilia genes were associated with a hypercoagulable state [5], [6], which may partly explain the development of preeclampsia. In recent decades, great attention has been paid to the role that thrombophilia genes may play in the development of preeclampsia. The aim of this meta-analysis was to evaluate the association between FVL or prothrombin G20210A polymorphism and preeclampsia.
In our meta-analysis, a 2-fold increased risk of preeclampsia and an approximately 3-fold increase for severe preeclampsia are observed when the prothrombin 20210A allele exists. After the exclusion of one study [10] the pooled OR for severe preeclampsia decreased markedly, although it was still statistically significant. The patients in this study seemed to have more severe disease with acute complications in comparison with other studies. After omission, the pooled OR decreased to 2.08, close to the pooled OR for all preeclampsia. This finding demonstrates that the roles played by prothrombin G20210A SNP in the increased risk of preeclampsia and severe preeclampsia may have no difference. Subgroup analyses of ethnicity were not conducted because of the lack of studies involving patients with genetic backgrounds other than Caucasian, which limited broadening the interpretation of our results to the general population.
These results are inconsistent with those of Lin and August [12], which revealed no significant associations. In Lin’s meta-analysis, a relatively small sample size (916 cases for all preeclampsia and 325 cases for severe preeclampsia) was collected in comparison with ours. It is suggested that the lack of statistical significance in the former meta-analysis might be due to the smaller number of studies. Therefore, our meta-analysis with a larger sample size (2296 cases for all preeclampsia and 1063 cases for severe preeclampsia) should give a more precise estimate under greater statistical power.
Our meta-analysis also indicates that FVL is associated with an increased risk of preeclampsia. The combined OR for FVL associated with all preeclampsia was 1.60 (95%CI 1.28–2.00), and the Q-statistic test suggested a mild heterogeneity between studies. The funnel plot was asymmetric, and the Egger test suggested obvious evidence of small-study bias. These results are similar to those of former meta-analyses [12], [53], and help to confirm that FVL may increase the risk of preeclampsia.
When the studies assessing the relationship between FVL and severe preeclampsia were involved in meta-analysis, there was a 2.45-fold increase in risk. High heterogeneity was found among all studies (I 2 = 56.1%, p = 0.003). This unexplained heterogeneity may be due to the wide variation of the prevalence of the FVL in the control populations. In most studies, the prevalence of FVL in the control group ranged from 2% to 5%, including all of the larger studies in this meta-analysis, All of them reported ORs much greater than 1. On the contrary, seven studies [16], [17], [22], [25], [35], [37], [48] had a higher prevalence of FVL in control groups (6.3%–13%), four of which reported ORs less than 1. After excluding the studies with a high FVL prevalence in control groups, the heterogeneity clearly decreased (I 2 = 25.1%, p = 0.212 versus I 2 = 56.1%, p = 0.003). The funnel plot showed no significant evidence of publication bias.
There are some limitations to our meta-analysis. First, the recruitment of patients and controls varied in different studies. In some studies the cases were matched with controls in several factors that may confound, e.g., age, weeks of gestation at delivery, systolic and diastolic blood pressure at <20 weeks’ gestation, and protein C deficiency, whereas in others they were not. These confounding factors may have added some bias to our analysis, although because the definition of preeclampsia and severe preeclampsia varied little in these studies, the selection bias would not be large. Second, because the majority of patients and controls come from the Caucasian population, our conclusion may not be applied to other populations and the general population. Although one study [28] has assessed this association in an Asian population, no conclusion was drawn due to the absence of FVL polymorphism in both case and control groups. It seems that this polymorphism is rarely detected in Asian population. Third, a moderate to high heterogeneity existed between the studies evaluating the association between FVL and severe preeclampsia, for which ethnic background explained little. Even though the heterogeneity decreased sharply after excluding studies with high FVL prevalence in control groups, it had nothing to do with the interpretation of results. More details are needed to analyze the source of heterogeneity. Last, there was some evidence of publication bias (i.e., lack of small negative studies) in our analysis. A larger sample size is essential for thorough meta-analysis, and more studies with small numbers of cases and controls recruited under the same inclusion criteria can help to decrease the publication bias.
In conclusion, these two thrombophilia gene polymorphisms, FVL and prothrombin G20210A, are associated with an increased risk of preeclampsia and severe preeclampsia, respectively. A large number of cases and controls are required to make a more precise risk estimate and minimize the bias in meta-analysis.
Supporting Information
PRISMA Checklist.
(DOC)
Acknowledgments
The authors acknowledge all the individuals who took part in this research, and also thank everyone who gave advice on data collection and analyses.
Funding Statement
This work was supported by the Knowledge Innovation Program of The Chinese Academy of Sciences (KSCX2-EW-R-06). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Sibai B, Dekker G, Kupferminc M (2005) Pre-eclampsia. Lancet 365: 785–799. [DOI] [PubMed] [Google Scholar]
- 2. Arngrimsson R, Hayward C, Nadaud S, Baldursdottir A, Walker JJ, et al. (1997) Evidence for a familial pregnancy-induced hypertension locus in the eNOS-gene region. Am J Hum Genet 61: 354–362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Wilson ML, Goodwin TM, Pan VL, Ingles SA (2003) Molecular epidemiology of preeclampsia. Obstet Gynecol Surv 58: 39–66. [DOI] [PubMed] [Google Scholar]
- 4. Preston FE, Rosendaal FR, Walker ID, Briet E, Berntorp E, et al. (1996) Increased fetal loss in women with heritable thrombophilia. Lancet 348: 913–916. [DOI] [PubMed] [Google Scholar]
- 5. Dahlback B (1994) Inherited resistance to activated protein C, a major cause of venous thrombosis, is due to a mutation in the factor V gene. Haemostasis 24: 139–151. [DOI] [PubMed] [Google Scholar]
- 6. Poort SR, Rosendaal FR, Reitsma PH, Bertina RM (1996) A common genetic variation in the 3′-untranslated region of the prothrombin gene is associated with elevated plasma prothrombin levels and an increase in venous thrombosis. Blood 88: 3698–3703. [PubMed] [Google Scholar]
- 7. Mimuro S, Lahoud R, Beutler L, Trudinger B (1998) Changes of resistance to activated protein C in the course of pregnancy and prevalence of factor V mutation. Aust N Z J Obstet Gynaecol 38: 200–204. [DOI] [PubMed] [Google Scholar]
- 8. Mello G, Parretti E, Martini E, Mecacci F, La Torre P, et al. (1999) Usefulness of screening for congenital or acquired hemostatic abnormalities in women with previous complicated pregnancies. Haemostasis 29: 197–203. [DOI] [PubMed] [Google Scholar]
- 9. Seremak-Mrozikiewicz A, Drews K, Wender-Ozegowska E, Mrozikiewicz PM (2010) The significance of genetic polymorphisms of factor V Leiden and prothrombin in the preeclamptic Polish women. J Thromb Thrombolysis 30: 97–104. [DOI] [PubMed] [Google Scholar]
- 10. Mello G, Parretti E, Marozio L, Pizzi C, Lojacono A, et al. (2005) Thrombophilia is significantly associated with severe preeclampsia: results of a large-scale, case-controlled study. Hypertension 46: 1270–1274. [DOI] [PubMed] [Google Scholar]
- 11. Salanti G, Sanderson S, Higgins JP (2005) Obstacles and opportunities in meta-analysis of genetic association studies. Genet Med 7: 13–20. [DOI] [PubMed] [Google Scholar]
- 12. Lin J, August P (2005) Genetic thrombophilias and preeclampsia: a meta-analysis. Obstet Gynecol 105: 182–192. [DOI] [PubMed] [Google Scholar]
- 13. ACOG technical bulletin. Hypertension in pregnancy. Number 219–January 1996 (replaces no. 91, February 1986). Committee on Technical Bulletins of the American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet 53: 175–183. [PubMed] [Google Scholar]
- 14. Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol 183: S1–S22. [PubMed] [Google Scholar]
- 15. Dizon-Townson DS, Nelson LM, Easton K, Ward K (1996) The factor V Leiden mutation may predispose women to severe preeclampsia. Am J Obstet Gynecol 175: 902–905. [DOI] [PubMed] [Google Scholar]
- 16. Kupferminc MJ, Eldor A, Steinman N, Many A, Bar-Am A, et al. (1999) Increased frequency of genetic thrombophilia in women with complications of pregnancy. N Engl J Med 340: 9–13. [DOI] [PubMed] [Google Scholar]
- 17. Kupferminc MJ, Fait G, Many A, Gordon D, Eldor A, et al. (2000) Severe preeclampsia and high frequency of genetic thrombophilic mutations. Obstet Gynecol 96: 45–49. [DOI] [PubMed] [Google Scholar]
- 18. Kupferminc MJ, Peri H, Zwang E, Yaron Y, Wolman I, et al. (2000) High prevalence of the prothrombin gene mutation in women with intrauterine growth retardation, abruptio placentae and second trimester loss. Acta Obstet Gynecol Scand 79: 963–967. [PubMed] [Google Scholar]
- 19. Fabbro D, D’Elia AV, Spizzo R, Driul L, Barillari G, et al. (2003) Association between plasminogen activator inhibitor 1 gene polymorphisms and preeclampsia. Gynecol Obstet Invest 56: 17–22. [DOI] [PubMed] [Google Scholar]
- 20. Driul L, Damante G, D’Elia A, Ianni A, Springolo F, et al. (2005) Genetic thrombophilias and uterine artery Doppler velocimetry and preeclampsia. Int J Gynaecol Obstet 88: 265–270. [DOI] [PubMed] [Google Scholar]
- 21. Hiltunen LM, Laivuori H, Rautanen A, Kaaja R, Kere J, et al. (2009) Blood group AB and factor V Leiden as risk factors for pre-eclampsia: a population-based nested case-control study. Thromb Res 124: 167–173. [DOI] [PubMed] [Google Scholar]
- 22. Tempfer CB, Jirecek S, Riener EK, Zeisler H, Denschlag D, et al. (2004) Polymorphisms of thrombophilic and vasoactive genes and severe preeclampsia: a pilot study. J Soc Gynecol Investig 11: 227–231. [DOI] [PubMed] [Google Scholar]
- 23. Davalos IP, Moran MC, Martinez-Abundis E, Gonzalez-Ortiz M, Flores-Martinez SE, et al. (2005) Methylenetetrahydrofolate reductase C677T polymorphism and Factor V Leiden variant in Mexican women with preeclampsia/eclampsia. Blood Cells Mol Dis 35: 66–69. [DOI] [PubMed] [Google Scholar]
- 24. Dalmaz CA, Santos KG, Botton MR, Tedoldi CL, Roisenberg I (2006) Relationship between polymorphisms in thrombophilic genes and preeclampsia in a Brazilian population. Blood Cells Mol Dis 37: 107–110. [DOI] [PubMed] [Google Scholar]
- 25. Gerhardt A, Goecke TW, Beckmann MW, Wagner KJ, Tutschek B, et al. (2005) The G20210A prothrombin-gene mutation and the plasminogen activator inhibitor (PAI-1) 5G/5G genotype are associated with early onset of severe preeclampsia. J Thromb Haemost 3: 686–691. [DOI] [PubMed] [Google Scholar]
- 26. Yalinkaya A, Erdemoglu M, Akdeniz N, Kale A, Kale E (2006) The relationship between thrombophilic mutations and preeclampsia: a prospective case-control study. Ann Saudi Med 26: 105–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. De Groot CJ, Bloemenkamp KW, Duvekot EJ, Helmerhorst FM, Bertina RM, et al. (1999) Preeclampsia and genetic risk factors for thrombosis: a case-control study. Am J Obstet Gynecol 181: 975–980. [DOI] [PubMed] [Google Scholar]
- 28. Kobashi G, Yamada H, Asano T, Nagano S, Hata A, et al. (1999) The factor V Leiden mutation is not a common cause of pregnancy-induced hypertension in Japan. Semin Thromb Hemost 25: 487–489. [DOI] [PubMed] [Google Scholar]
- 29. Prasmusinto D, Skrablin S, Fimmers R, van der Ven K (2004) Ethnic differences in the association of factor V Leiden mutation and the C677T methylenetetrahydrofolate reductase gene polymorphism with preeclampsia. Eur J Obstet Gynecol Reprod Biol 112: 162–169. [DOI] [PubMed] [Google Scholar]
- 30. Faisel F, Romppanen EL, Hiltunen M, Helisalmi S, Laasanen J, et al. (2004) Susceptibility to pre-eclampsia in Finnish women is associated with R485K polymorphism in the factor V gene, not with Leiden mutation. Eur J Hum Genet 12: 187–191. [DOI] [PubMed] [Google Scholar]
- 31. Dusse LM, Carvalho M, Braganca WF, Paiva SG, Godoi LC, et al. (2007) Inherited thrombophilias and pre-eclampsia in Brazilian women. Eur J Obstet Gynecol Reprod Biol 134: 20–23. [DOI] [PubMed] [Google Scholar]
- 32. Kim YJ, Williamson RA, Murray JC, Andrews J, Pietscher JJ, et al. (2001) Genetic susceptibility to preeclampsia: roles of cytosineto-thymine substitution at nucleotide 677 of the gene for methylenetetrahydrofolate reductase, 68-base pair insertion at nucleotide 844 of the gene for cystathionine beta-synthase, and factor V Leiden mutation. Am J Obstet Gynecol 184: 1211–1217. [DOI] [PubMed] [Google Scholar]
- 33. Demir SC, Evruke C, Ozgunen T, Kadayifci O, Altintas U, et al. (2006) The relationship between pregnancy induced hypertension and congenital thrombophilia. Saudi Med J 27: 1161–1166. [PubMed] [Google Scholar]
- 34. Aggarwal S, Dimri N, Tandon I, Agarwal S (2011) Preeclampsia in North Indian women: the contribution of genetic polymorphisms. J Obstet Gynaecol Res 37: 1335–1341. [DOI] [PubMed] [Google Scholar]
- 35. Malek-Khosravi S, Rahimi Z, Jalilvand F, Parsian A (2012) Thrombophilic mutations and susceptibility to preeclampsia in Western Iran. J Thromb Thrombolysis 33: 109–115. [DOI] [PubMed] [Google Scholar]
- 36. Hira B, Pegoraro RJ, Rom L, Moodley J (2003) Absence of Factor V Leiden, thrombomodulin and prothrombin gene variants in Black South African women with pre-eclampsia and eclampsia. BJOG 110: 327–328. [PubMed] [Google Scholar]
- 37. Currie L, Peek M, McNiven M, Prosser I, Mansour J, et al. (2002) Is there an increased maternal-infant prevalence of Factor V Leiden in association with severe pre-eclampsia? BJOG 109: 191–196. [DOI] [PubMed] [Google Scholar]
- 38. Livingston JC, Barton JR, Park V, Haddad B, Phillips O, et al. (2001) Maternal and fetal inherited thrombophilias are not related to the development of severe preeclampsia. Am J Obstet Gynecol 185: 153–157. [DOI] [PubMed] [Google Scholar]
- 39. von Tempelhoff GF, Heilmann L, Spanuth E, Kunzmann E, Hommel G (2000) Incidence of the factor V Leiden-mutation, coagulation inhibitor deficiency, and elevated antiphospholipid-antibodies in patients with preeclampsia or HELLP-syndrome. Hemolysis, elevated liver-enzymes, low platelets. Thromb Res 100: 363–365. [DOI] [PubMed] [Google Scholar]
- 40. van Pampus MG, Dekker GA, Wolf H, Huijgens PC, Koopman MM, et al. (1999) High prevalence of hemostatic abnormalities in women with a history of severe preeclampsia. Am J Obstet Gynecol 180: 1146–1150. [DOI] [PubMed] [Google Scholar]
- 41. O’Shaughnessy KM, Fu B, Ferraro F, Lewis I, Downing S, et al. (1999) Factor V Leiden and thermolabile methylenetetrahydrofolate reductase gene variants in an East Anglian preeclampsia cohort. Hypertension 33: 1338–1341. [DOI] [PubMed] [Google Scholar]
- 42.Kahn SR, Platt R, McNamara H, Rozen R, Chen MF, et al.. (2009) Inherited thrombophilia and preeclampsia within a multicenter cohort: the Montreal Preeclampsia Study. Am J Obstet Gynecol 200: 151 e151–159; discussion e151–155. [DOI] [PubMed]
- 43. Higgins JR, Kaiser T, Moses EK, North R, Brennecke SP (2000) Prothrombin G20210A mutation: is it associated with pre-eclampsia? Gynecol Obstet Invest 50: 254–257. [DOI] [PubMed] [Google Scholar]
- 44. D’Elia AV, Driul L, Giacomello R, Colaone R, Fabbro D, et al. (2002) Frequency of factor V, prothrombin and methylenetetrahydrofolate reductase gene variants in preeclampsia. Gynecol Obstet Invest 53: 84–87. [DOI] [PubMed] [Google Scholar]
- 45. Morrison ER, Miedzybrodzka ZH, Campbell DM, Haites NE, Wilson BJ, et al. (2002) Prothrombotic genotypes are not associated with pre-eclampsia and gestational hypertension: results from a large population-based study and systematic review. Thromb Haemost 87: 779–785. [PubMed] [Google Scholar]
- 46. Prochazka M, Krcova V, Kudela M, Slavik L (2003) [Occurrence of gene mutations in factor V Leiden, prothrombin and methylenetetrahydrofolate reductase in patients with pre-eclampsia]. Ceska Gynekol 68: 162–166. [PubMed] [Google Scholar]
- 47. Best LG, Dorsam ST, Nadeau M, Burd L, Anderson CM (2009) Genetic thrombophilia variants and risk for preeclampsia among American Indians. Hypertens Pregnancy 28: 85–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Alfirevic Z, Mousa HA, Martlew V, Briscoe L, Perez-Casal M, et al. (2001) Postnatal screening for thrombophilia in women with severe pregnancy complications. Obstet Gynecol 97: 753–759. [DOI] [PubMed] [Google Scholar]
- 49. Koleva R, Dimitrova V, Chernev T, Savov A, Karag’ozova Z, et al. (2005) [Impact of inherited thrombophilia on the development of some pregnancy complications]. Akush Ginekol (Sofiia) 44: 18–26. [PubMed] [Google Scholar]
- 50. Lindoff C, Ingemarsson I, Martinsson G, Segelmark M, Thysell H, et al. (1997) Preeclampsia is associated with a reduced response to activated protein C. Am J Obstet Gynecol. 176: 457–460. [DOI] [PubMed] [Google Scholar]
- 51. Dissanayake VH, Sirisena ND, Weerasekera LY, Gammulla CG, Seneviratne HR, et al. (2012) Candidate gene study of genetic thrombophilic polymorphisms in pre-eclampsia and recurrent pregnancy loss in Sinhalese women. J Obstet Gynaecol Res 38: 1168–1176. [DOI] [PubMed] [Google Scholar]
- 52. Rigo J Jr, Nagy B, Fintor L, Tanyi J, Beke A, et al. (2000) Maternal and neonatal outcome of preeclamptic pregnancies: the potential roles of factor V Leiden mutation and 5,10 methylenetetrahydrofolate reductase. Hypertens Pregnancy 19: 163–172. [DOI] [PubMed] [Google Scholar]
- 53. Dudding T, Heron J, Thakkinstian A, Nurk E, Golding J, et al. (2008) Factor V Leiden is associated with pre-eclampsia but not with fetal growth restriction: a genetic association study and meta-analysis. J Thromb Haemost 6: 1869–1875. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
PRISMA Checklist.
(DOC)