
Fig. 14.
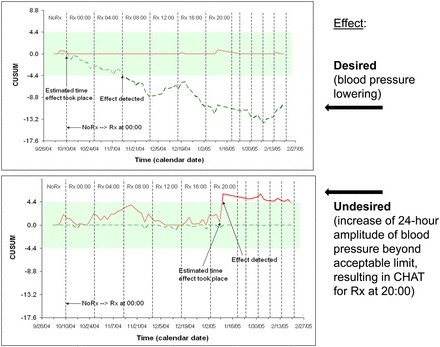
Top: changing timing of medication (ΔRx) during consecutive spans shows efficacy of treatment. An empirical approach to chronotherapy: immediately after diagnosis, one should ascertain that the treatment is effective. Optimization of treatment effects by timing can be achieved for the individual patient by systematically changing, e.g., advancing the time of treatment. Successful treatment of MH assessed by a self-starting cumulative sum (CUSUM) control chart. To optimize his hypotensive treatment (Rx), a just-diagnosed 24-yr-old individual (T.T.) switched his Rx first every 17 days by 4 h and then mostly at shorter intervals. Note statistically significant decrease in MESOR, evidenced by the breakout outside the decision interval of the negative CUSUM line. With continued Rx, the BP MESOR leaves the decision interval, indicating a statistically significant decrease in overall blood pressure. Bottom: changing timing of medication (ΔRx) during consecutive spans shows risk of iatrogenic CHAT. An empirical approach to chronotherapy: immediately after diagnosis, one should ascertain that one does not induce CHAT by inappropriate timing of antihypertensive medication. In this 24-yr-old man (T.T.) who advanced the time of treatment by 4 h every 17 days initially and at shorter intervals thereafter, treatment in the evening was associated with iatrogenic CHAT, raising the question whether the risk of MH may not have been traded for the even higher risk of stroke that CHAT represents. Iatrogenic CHAT, induced by treatment at 20:00 daily, was silent to office visits. T.T. may have traded benefit (lowering of the MESOR of BP, top) for something worse (CHAT). This danger applies to some patients with hypertension (who tend to have a large circadian amplitude of blood pressure) to whom treatment time is not specified (or is specified for bedtime) by the care provider, as was the case for T.T. A few others who took hypertensive medication at bedtime were also found to have CHAT. The figure shows the assessability of otherwise undetected harm by as-one-goes sequential analysis.