
Figure 5.
TREML4 Localization in Human Coronary Atheroma
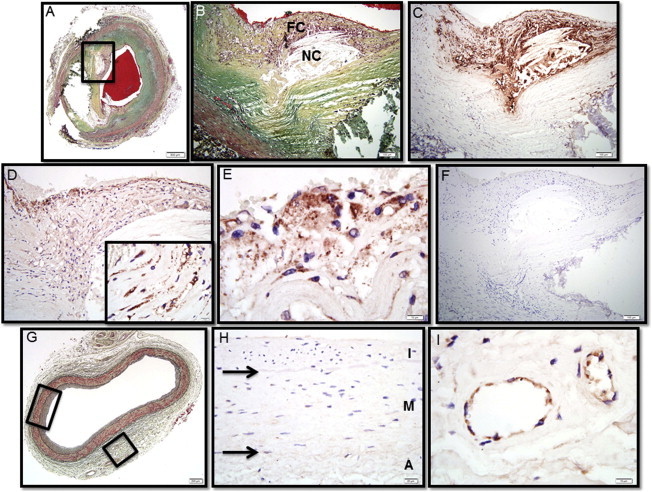
(A) Human coronary fibroatheroma with calcification, Movat pentachrome stain. The red area in the central lumen is the postmortem clot.
(B) A high-power magnification of the area within the black box in (A) showing a necrotic core (NC) rich in free cholesterol with an overlying thin fibrous cap (FC) infiltrated by inflammatory cells.
(C) Immunostaining with the macrophage marker CD68 shows extensive reactivity in the fibrous cap and surrounding necrotic core.
(D) Immunostaining with a rabbit polyclonal antibody targeted against TREML4 is strongly positive in the superficial region of the fibrous cap and perinecrotic core (inset).
(E) A high-power magnification of region shown in (D) shows intense TREML4 staining of inflammatory cells bordering the luminal space.
(F) The adjacent histologic section immunostained with nonspecific anti-rabbit antisera shows negative staining.
(G) A control artery from the same patient exhibiting adaptive intimal thickening, Movat pentachrome stain.
(H) A high-power view of the section in (G) shows negative staining for TREML4 (A, tunica adventitia; M, tunica media; and I, tunica intima).
(I) The same section as (G) showing positive staining for TREML4 in adventitial vasa vasorum.
Scale bars represent 500 μm (A); 100 μm (B–D, F); 200 μm (G); 20 μm (H); or 10 μm (insets in D, E, I).